Download

1 / 46
2.45k likes | 8.52k Views
Rickets. Definition of Rickets. Rickets, a disease of growing bone , occurs in children only before fusion of the epiphyses, and is due to unmineralized matrix at the growth plates.

E N D
Definition of Rickets Rickets, a disease of growing bone, occurs in children only before fusion of the epiphyses, and is due to unmineralized matrix at the growth plates.
Proper bone formation requires a complex interplay of several organs and chemicals and vitamin D deserves special mention because any disturbance in its production, absorption, or metabolism is paramount in the development of rickets.
Human beings maintain adequate levels of vitamin D by producing it from cholesterol or by absorbing it from ingested food sources. • Sunlight is a vital component necessary for the production of vitamin D, which begins in the skin and ends in the kidney .
Functions of Chemicals Involved in Bone Formation: • Alkaline phosphatase: Exact function unknown; isoenzyme is elevated in conditions such as rickets that are associated with high bone turnover.
Functions of Chemicals Involved in Bone Formation: • Calcitriol: Bone: indirectly stimulates bone synthesis via increased calcium absorption in intestinal lumen. Intestine: increases calcium, phosphorus, and magnesium absorption. Kidney: autoregulation of calcitriol production by the kidney. Parathyroid gland: negative feedback to decrease secretion of parathyroid hormone.
Functions of Chemicals Involved in Bone Formation: • Parathyroid hormone: Bone: mobilizes calcium and phosphorus. Intestine: indirectly increases calcium and phosphorus absorption by increasing calcitriol. Kidney: increases 1,25OHvit D, increases calcium reabsorption, decreases phosphorus reabsorption.
Radiological findings: 1- Widening ,Fraying, Cupping صفحه رشداپی فيزی 2- کاهش مينراليزاسيون صفحه رشد 3- Translucent gap بين اپی فيز و متافيز 4- ظهور اپی فيز به تاخير می افتد، اپی فيز کوچک 5- Cupping و Widening متافيز باعث می شود که نسج نرم انتهای استخوانExpansionپيدا کند و برجسته و متورم به نظر برسد.(Rickets Rosary)، پهن شدن مچ دست و قوزک. 6- کورتکس نازک 7- استئوپنی 8- ترابکولهای استخوانی کم و خشن
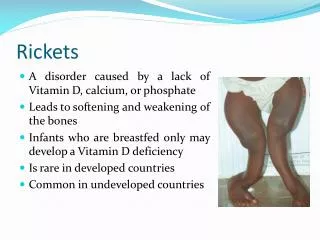
CLINICAL MANIFESTATIONS: • Delay in the closure of the fontanelles • Parietal and frontal bossing (caput quadratum) • Craniotabes (soft skull bones) • Rachitic rosary • Harrison sulcus • Enlargement of the wrist and bowing of the distal radius and ulna • Progressive lateral bowing of the femur and tibia
CLINICAL MANIFESTATIONS: • Hypoplasia of the dental enamel . • Decreased muscle tone, leading to delayed achievement of motor milestones . • Hypocalcemic seizures (frequent presenting sign in the first year of life ) . • Prone to acquiring infectious diseases . • Increased sweating is a common finding in young infants .
Skeletal and Radiographic Findings Associated with Rickets: • Flaring of wrists . • Fractures. • Fraying and cupping of metaphysis . • Frontal bossing of skull . • Genu valgum or varum. • Lordosis/kyphosis/scoliosis . • Osteopenia
Types of Rickets: • Nutritional rickets • Vitamin D-dependent rickets • Familial hypophosphatemic rickets • Hereditary hypophosphatemic rickets with hypercalciuria • Other causes of rickets include renal disease, medications, and malabsorption syndromes.
Nutritional Rickets: • Nutritional rickets results from inadequate sunlight exposure or inadequate intake of dietary vitamin D, calcium, or phosphorus . • Vitamin D deficiency can occur when an infant is solely breastfed, is dark skinned, or has limited sunlight exposure . • Breast milk content of vit D: 12 – 60 IU/lit
Nutritional Rickets: • Nutritional rickets presents in the first two years of life with short stature, gait abnormality, developmental delay, and characteristic findings. • Commonly, infants younger than six months present with hypocalcemictetany or seizures, whereas older children present with failure to thrive or skeletal deformities .
VITAMIN D–DEPENDENT RICKETS, TYPE 1: • Autosomal recessive • Mutation in gene of renal 1α-hydroxylase • They present during the 1st 2 yr of life. • Biochemical finding : 25-D …. normal 1,25-D…. decreased PTH…. increased Ph…. decreased ca…. decreased metabolic acidosis • The only form of richets with hypocalcemia.
VITAMIN D–DEPENDENT RICKETS, TYPE 2: • Autosomal recessive • Mutation in gene of vitamin D receptor. • Levels of 1,25-D are extremely elevated • Approximately 50–70% of children have alopecia(areata or totalis).
X-LINKED HYPOPHOSPHATEMIC RICKETS: • Pathophysiology: The defective gene is called PHEX. This gene have a role in inactivating phosphatonin. increased phosphate excretion.
Hypophosphatemia also can occur secondary to hereditary hypophosphatemic rickets with hypercalciuria, which is believed to result from an isolated defect in renal reabsorption of phosphorus .
Other Causes: • Medications: Antacids Anticonvulsants Corticosteroids Loop diuretics • Malignancy • Prematurity
Tumor-induced osteomalacia: • This is more common in adults. • In children, it produce classic rachitic findings. • The tumors are benign, small, and located in bone.
Other Causes: • Diseases of organs associated with vitamin D and calcium metabolism : Kidney disease Liver and biliary tract disease • Malabsorption syndromes : Celiac disease Cystic fibrosis (rare)
Premature infants are at risk of developing rickets from calcium and phosphorus deficiency and side effects of their medications (e.g., loop diuretics, corticosteroids) .
MEDICAL HISTORY: • The infant's gestational age, diet, and degree of sunlight exposure should be noted . • A detailed dietary history should include specifics of vitamin D and calcium intake . • A family history of short stature, orthopedic abnormalities, poor dentition, alopecia, and parental consanguinity may signify inherited rickets .
MEDICAL HISTORY: • Researchers have suggested an appropriate amount of sunlight exposure for infants (i.e., 30 minutes per week if only in a diaper and two hours per week if fully clothed), but the exact amount needed for a particular child is not known . (J Pediatr 1985;107:372-6 )
Physical Examination: • In children with rickets, complete physical and dental examinations should be performed . • The entire skeletal system must be palpated to search for tenderness and bony abnormalities . • Bowlegs in the absence of other findings are relatively commonin normal children in the first two years of life.
Nutritional Rickets: • Treatment:vitamin D nutritional intake of ca There are 2 strategies for administration of vitamin D: a)In first year 100,000-200,000 IU vit D orally or im b)After 1 year 300,000–600,000 IU vit D orally o im alternative : 2,000–5,000 IU/day over 4–6 wk.
:تغييرات بيوشيميايی پس از درمان • کلسيم در عرض 3 روز نرمال می شود. • فسفر آخر هفته اول نرمال می شود. • آلکالن فسفاتاز چندين هفته تا ماه بالا باقی می ماند ، به طور معمول 6 تا 12 ماه بعد کاهش می يابد. • بهبودی علائم راديولوژی 2 هفته دير تر از تغييرات بيوشيميايی رخ می دهد.
Vitamin D-dependent Rickets: • Because vitamin D-dependent rickets, type I is caused by lack of production of calcitriol, treatment requires the replacement of that active product. (calcitriol:0.25-2μg/day)
Treatment: The treatment of type II is more complex 1)high-dose vitamin D(vitamin D2, 25-D, or 1,25-D) 50-60 μg/day 1,25-D 2)oral calcium (1–3 gr/day) • If do not respond to high-dose vitamin D : long-term Iv calcium, with transition to very high-dose oral calcium.
Familial hypophosphatemic Rickets: • Familial hypophosphatemic rickets is treated with oral phosphorus and calcitriol (Rocaltrol). • Hereditary hypophosphatemic rickets with hypercalciuria requires replacement of oral phosphorus alone. • Joulie's solution (155 g of dibasic anhydrous sodium phosphate and 64 g of phosphoric acid 85 percent per liter solution, corresponding to 50 mg/mL of elemental phosphorus).
Treatment: • oral phosphorus (1–3 g of elemental phosphorus divided into 4–5 doses ) & • 1,25-D (calcitriol 30–70 ng/kg/day divided into 2 doses ). • growth hormone (significant short stature)
Rickets associated with anticonvulsants: • Needs 1000 and sometimes 4000 IU /day vit D.
Oncogenic rickets: • excision of the tumor. If cannot be removed, treatment is identical to that used for XLH.
KEY RECOMMENDATIONS FOR PRACTICE: • Surgical intervention may be necessary to repair severe bony abnormalities in children with rickets, but it should not be undertaken until the biochemical derangements have resolved so that optimal healing occurs at the surgical site .
Differential Diagnosis Metaphyseal dysplasia: • Bowing of legs. • Short stature. • Waddling gait. • Normal level of Ca,Ph,alkaline phosphatase. • Cupped or ragged metaphyses. • Jansen type & Schmid type.
Differential Diagnosis: Hypophosphatasia : • X-ray resembles rickets. • Low level of alkaline phosphatase.