Download
1 / 27
270 likes | 551 Views
Office Vocal Cord Injections: Applying bioengineered products to classic laryngologic problems. Matthew Lutch, MD Head and Neck Surgery Kaiser Permanente Medical Center San Diego, California . Medialization Procedures.

E N D
Office Vocal Cord Injections:Applying bioengineered products to classic laryngologic problems Matthew Lutch, MD Head and Neck Surgery Kaiser Permanente Medical Center San Diego, California
Medialization Procedures • Terminology often unclear • Open vs endoscopic • Office-based vs operating room • Thyroplasty vs laryngoplasty • Injectable implants vs permanent implants • Implantable implants? • Laryngoplasty is catch-all • Thyroplasty reserved for open procedures • Injection laryngoplasty (IL)/vocal fold injection (VFI)
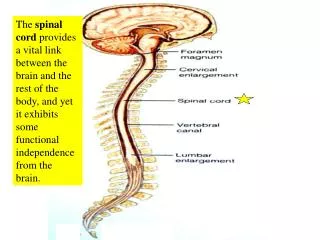
Vocal Fold Injection • Classic Laryngologic Problems • Glottic insufficiency catches all • Vocal fold paralysis/paresis • Tissue loss (neoplasm/trauma) • Presbylarynx (subset) • Loss of superficial lamina propria • Sulcus vocalis
Classics in VFI • Brünings, 1911 • paraffin • Arnold, 1963 • Teflon • All initially “office-based” • Awake, upright patients
Manuel Garcia: Observations on the human voice. Proc Royal Soc London. 1855;7:397-410
Technique • Mirror guided surgery • General anesthesia • Standard of care ~1960 • Priest, et al. Direct laryngoscopy under general anesthesia. Trans Am Acad Opthamol Otolaryngol. 1960;64:639-48. • Scalco, et al. Microscopic suspension laryngoscopy. Ann Otol Rhinol Laryngol. 1960;69:1134-8.
What awake VFI offers • Shorter “down-time” • Decreased cost (RVUs!) • “Real-time” feedback • Addresses specific anatomic problem • More customized therapy • Multiple bioengineered injectable options • Open thyroplasty - OR mandated
Disadvantages of VFI • Preprocedure anxiety • Intraprocedural gagging • Cannot guarantee longevity of implant • Precision of injection α patient comfort
Injectable options • Duration, viscosity, inflammatory risk • Saline • Gelfoam • Restylane/Juvederm • Collagen • Fat • Artecoll/Teflon/Radiesse (CaHA)
Why hyaluronic acid? • The “goo” molecule • Carbohydrate polymer • Extracellular matrix (15 grams/70 kg) • Natural lubricant (synovial fluid) • Cross-linking increases longevity
Juvederm Ultra series • 34 patients • 4 required repeat injection x 1 • 1 required repeat injection x 2 • 5 bilateral injectees • 45 total injections
Patient population GLOTTIC INSUFFICIENCY CATCHES ALL… • Idiopathic -12 • Lung cancer – 4 • Thyroid cancer – 3 • Esophageal cancer 2 • Metastatic breast - 2 • Presbylarynx – 5 • Chondrosarcoma – 1 • Jugular foramen schwannoma – 1 • Carotid endarterectomy – 3 • Cricoarytenoid joint fixation - 1
Awake approaches • Real time voice/visual feedback • Transoral* • Duplicates approach of direct laryngoscopy • Difficult in the gagging patient • Percutaneous • Transcricothyroid • Transthyrohyoid • Requires MD or SLP to drive scope • Optimal in gagging patient
Technique of transoral injection • Base of tongue directly topicalized • Cetacaine • Methemoglobinemia • Atomized 4% lidocaine treatment • Direct glottic topicalization
Case #1 • 55 year old man s/p open resection of chondrosarcoma • Substantial glottic insuffiency secondary to loss of paraglottic tissue and RLN sacrifice
Preinjection stroboscopy film 1AInjection film 1BPostinjection (6m) stroboscopy 1C
Case #2 • 79 year-old with dysphonia after left carotid endarterectomy • Left vocal fold paralysis and left sulcus vocalis deformity • Injection addresses both
RW2A – preinjection strobeRW2B – injection/multiple passesRW2C – postinjection strobe
Case #3 • 70 year old jewelry salesman • Breathy dysphonia s/p CABG • Intubated with 8.5 endotracheal tube
JHpresby3A: preinjection strobeJHpresby3B: bilateral vfiJHpresby3C: postinjection strobe
Followup • 1 to 17 months • 5 patients required repeat injection • 1 underwent open thyroplasty
Summary • Rejuvenating time-honored approaches • More options for patients • Decreased downtime • Minimal risk • Followup driven by patients: