Download
1 / 29
310 likes | 820 Views
Preterm Labour and PPORM. Dr. Yasir Katib MBBS, FRCSC Perinatologest. Outline. Definition Burden of Illness Etiology & Risk Factors Diagnosis Management ?tocolytics ?antibiotics steroids. Preterm Labour: Definition.

E N D
Preterm Labour andPPORM Dr. Yasir Katib MBBS, FRCSC Perinatologest
Outline • Definition • Burden of Illness • Etiology & Risk Factors • Diagnosis • Management • ?tocolytics • ?antibiotics • steroids
Preterm Labour: Definition • Regular uterine contractions + progressive cervical dilatation and/or effacement at < 37 weeks GA
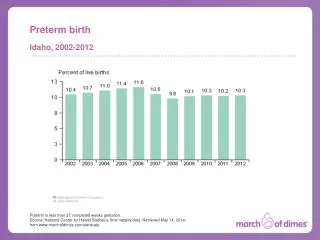
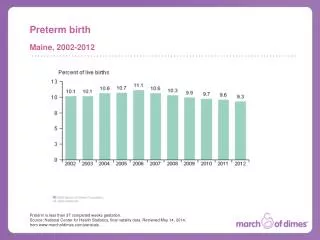
Burden of Illness: Incidence • Preterm delivery occurs in 12% pregnancies • 3-4% were <34 weeks • Those > 34 weeks born in tertiary care centres have survival rates = term • Long-term sequelae mainly in those born < 34 weeks • 70-80% occur spontaneously
Burden of Illness: Significance • Preterm birth accounts for 75% of Perinatal mortality • Long-term sequelae include: • CNS & neurodeveopmental problems • respiratory • blindness and deafness • Significant physical psychological and financial burdens
Long-term Morbidity of Extreme PTD MUMC < 29 weeks GA 1983 - 1988 n = 464 44% 50% 40% 31% 27% 30% 22% 20% 11% 9% 10% 0% 23 24 25 26 27 28 Gestational Age at Birth (weeks)
Etiology & Risk Factors • Idiopathic • PPROM • Antepartum hemorrhage • Chorioamnionitis • Multiple pregnancy/polyhydramnios • Incompetent cervix/uterine anomaly • Maternal disease • Fetal Anomaly
Prevention • No benefit has been demonstrated by attempts to prevent PTL with: • social interventions • bed rest • methods of cervical assessment • medications including betamimetics, magnesium, calcium • May be some increase in gestation with: • fish oil • progesterone injections • (need further study of both to show benefit)
Diagnosis • Establish Due Date • Naegele’s Rule • U/S • 7-12 weeks: +/- 5d • 13-21 weeks: +/- 1wk • 22-30 weeks: +/- 2wk • 30+ weeks: +/- 3wk • (document clearly on assessments!)
Diagnosis • History of contractions / risk factors • Abdo exam for contractions • Cervical exam – serial if necessary • 20-50% preterm labour diagnosis is incorrect • Vaginal fibronectin • Cervical U/S
Management • Four Objectives: • 1. Early diagnosis • 2. ID and treat cause if possible • 3. Attempt to arrest Labour when appropriate • 4. Minimize neonatal morbidity and mortality
Management Medications MgSO4 Ca channel blockers Cyclo-oxygenase inhibitors Oxytocin receptors antagonists Nitric oxcide
Arresting Labour • Note: <40% patients in preterm labour are candidates for tocolysis • Goal of tocolysis: • get 48 hrs for steroids to have effect • transport
Tocolysis • When NOT to tocolyse: • significant vaginal bleeding • suspected fetal asphyxia • intraamniotic infection • IUFD or lethal anomaly • maternal indication • imminent delivery
Tocolysis: Options • ECPC: • no effect: • fluid bolus • ethanol • sedation • magnesium sulphate
Tocolysis • ECPC: • Some effect: • betamimetics • calcium channel blockers • indomethacin • antimicrobials • oxytocin antagonists
Antimicrobials: ORACLE II • Kenyon et al. Lancet 2001 Mar 31;357(9261):989-94 • Methods: • multicentre randomised controlled trial • 6295 women in preterm labour (diagnosis left to individual clinician) w/ IM, no evid infection & “substantial uncertainty as to whether antbiotics should be prescribed” • randomized to: • erythromycin • co-amoxiclav • both • placebo
ORACLE II • Conclusion: • Abx should not be routinely prescribed in PTL w/o evidence of infection or PPROM
Effect of Corticosteroids on Neonatal Outcomes RDS IVH NEC Perinatal Infection Neonatal Death 0.1 1 10 Odds Ratio (95% Confidence Interval) Crowley CCPC Review No. 02955
Recommendations: NIH • NIH Consensus Statement JAMA Feb. 1, 1995 273:5:411-417. • fetuses 24-34 weeks w/ threatened PTL candidates for corticosteroids • pts eligible for toco should be eligible for steroids • Tx: betamethasone 12mg IM Q 24hr x 2 • Dexamethasone 6 mg IM Q 12 hr x 4 • Max benefit 24 hr – 7d, but.. • Give even if delivery anticipated w/in 24 hrs b/c some still beneficial
Upper Gestational Limit • NIH 1995: give steroids to 24-34wks (adopted by SOGC 1995) • ALARM: 34-36 wks • UK Royal College of Obs and Gyn: up until 36 wks
100 80 60 RDS (%) 40 20 0 20 24 28 32 36 40 Gestational age (weeks) RDS - Incidence
GBS PROPHYLAXIS • The benefits of group B streptococcal (GBS) prophylaxis are well established. • Intrapartum prophylaxis should be initiated in any patient with an unknown GBS status or a history of a positive culture during the present pregnancy. • Treatment is not indicated if there was a recent negative anovaginal culture
The effect of antibiotics on GBS Reduction ratio in GBS colonization after a single 2gm dose of IV ampicillin Time
Take home points • Accurate diagnosis key • Dating • Really labour? • Tocolysis (where appropriate) • choices • Ca channel blocker • goals: • give corticosteroids (once) • transfer to appropriate level facility • To reduce neonatal mortality & morbidity: • Steroids