Download
1 / 14
160 likes | 329 Views
MANAGING A CONTINUUM OF CARE WITH REVOLVING DRUG FUND FOR PEOPLE WITH DIABETES (DM) AND HYPERTENSION (HBP) THROUGH A PEER EDUCATOR NETWORK IN RURAL CAMBODIA. Maurits VAN PELT MAO Ngeav. Abstract.

E N D
MANAGING A CONTINUUM OF CARE WITH REVOLVING DRUG FUND FOR PEOPLE WITH DIABETES (DM) AND HYPERTENSION (HBP) THROUGH A PEER EDUCATOR NETWORK IN RURAL CAMBODIA MauritsVAN PELT MAO Ngeav
Abstract Problem statement: No affordable care model meets the secondary prevention needs of chronic NCD patients in developing countries. The great majority of Cambodian DM and HBP patients lack a continuum of care and access to routine prescription medicines. Objectives: To document how a peer educator network (PEN) in a rural Cambodian district delivers an affordable and acceptable continuum of care that includes prescription drugs to its community of DM and HBP patients Design: Intervention effects (before and after, no control group) Setting: A rural district of 133,000 inhabitants mostly served by private health services and to a lesser extent by public health services Study population: 1,023 chronic patients among whom 448 have DM Intervention: During 3.5 years, a network of 9 community-based diabetic peer educators (PEs) organizes self-screening of the adult population, first for DM and later also for HBP. To patients who register as members, the PEN delivers a continuum of care consisting of education on lifestyle changes, DM, and HBP self-management skills and materials, as well as information on how to access routine medication from the RDF and other services. PEs do not prescribe medicines, but rather facilitate access to professional health services, such as laboratory tests and medical consultation, when needed. Individual PE performance is assessed twice a year, providing data for quality control and learning opportunities. Contracted private pharmacies sell RDF medicines to members based on physician prescriptions and allow monitoring of treatment adherence by registered members. The laboratory services as well as drug sales generate revenue for replenishment of stocks, payment of PE incentives, re-supply of PEs with consumables, supervision of PEs, and assessments; they also pay part of the management costs. Outcome measure(s) and results: Results are given in numbers and percentage by gender. The 65% female DM and 35% male DM patients used medical consultation in equal proportions: 3.4 times in 2010. Among HBP patients, 63% are women. Reported health expenditure among DM was equivalent to USD 3.69 per month. Fasting blood glucose assessed per July 2010 in a randomly selected sample of 114 DM patients was 145 mg/dl on average, down from their baseline value of 191 mg/dl. 48% of DM patients showed FBG of ≤126 mg/dl (7 mmol). In the same sample, the proportion of DM patients with systolic blood pressure <130 mm Hg had increased from 42% in the baseline to 50%; whereas diastolic pressure <80 mm Hg had increased from 32% at baseline to 52%. The proportion of DM patients with normal BMI values (18.5–23.0) improved from 36% to 41%. The average annual drop-out rate of the DM group was just below 10%. 81% of DM patients reported that they felt better than before registration and >90% reported that they were satisfied with their peer educator. Revenue from providing laboratory services and medicine sales cover the local costs of running the PEN, but not the NGO management costs. HBP patients were only registered in year 3 and have begun to benefit from the system. The intervention is being replicated to other districts in the same province. Conclusion: In Cambodia, despite few resources, a PEN can deliver secondary prevention services including access to routine medication for DM and HBP patients. Generated service revenue can cover the running costs of a continuum of care. If trained and supervised, DM and HBP patients can fill certain gaps in services by taking on caregiver tasks. Three years onward, the PEN performs a range of effective secondary prevention measures for DM and HBP patients at low cost that is affordable to many of its members. The main lesson is that a structured membership of chronic NCD patients can trigger and maintain a matching demand for and supply of health services including medicines, making the rural health system more complete and responsive and bringing universal coverage closer in view of rapidly growing health needs.
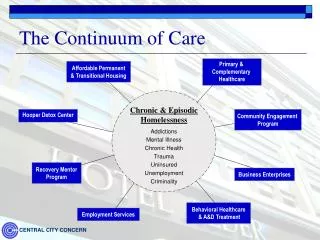
Background 1 • As Cambodian primary care is designed to deliver only acute care, it lacks routine medication and care for patients with chronic NCD such as Diabetes (DM) and hypertension (HBP). • Shifting public health tasks to paid Peer Educators (PE) creates additional human resources who fill the gap in services and help to deliver not just a responsive and affordable “continuum-of-care” that includes routine medication, which is unnecessarily expensive in the private sector and often not available. • Since 2005 a Cambodian NGO trains selected DM patients to become community-based PE who create their local networks of patients. • Organised into district Peer Educator Networks these PE detect and register other DM and HBP patients as member, entitling them to the continuum of care the delivery of which PE actively facilitate and of which PE are themselves users being chronic patients.
Background 2 Patient Membership : Once a patient is detected in the community covered by the PE, he/she can register (for free) as member of the network. This membership entitles her or him to counselling, diagnostic tests, diabetes education, follow-up, (paid) outpatient medical consultation and (paid) routine medication from the Revolving Drug Fund (RDF). More than 2/3 of registered DM patients are women. 29% of DM patients is older than 60 years (compared to 6.6% in the total rural Cambodian population). Peer Educators: Their number in the study district has grown from 1 to 8 between mid 2007 and mid 2009. In this district, there is one peer educator who covers 2 health center areas instead of only one. Only 1/3 of PE are women.
Objective / Study Questions • OBJECTIVE: To document how a peer educator network (PEN) in a rural Cambodian district delivers an affordable and acceptable continuum-of-care that includes prescription drugs to its community of DM and HBP patients. • Study Questions: • How can rural Cambodian DM and HBP be diagnosed earlier at low cost? • What are the 3-year outcomes of community-based diabetic PE helping other DM patients cope better with chronic disease? • How can a cost effective continuum of care that includes routine medication be made affordable and sustainable in a low resource setting such as in rural Cambodia?
Methods 1 1) We use the Cambodian STEP Survey results on prevalence of 2010 and routine registration data collected from detected DM patients to calculate the effectiveness of detection of DM. 2a) Upon registration the PE assess every new patient filling a form recording body weight, height, waist- and hip circumference, blood pressure, blood sugar values, pulse, signs of secondary complications, personal- and socio-economic data including when they were first told they have DM or HBP and who had first diagnosed them; 2b) Twice per year, as part of routine monitoring the NGO selects a random sample of 19 diabetes patients per PE among those who have been followed-up for more than 6 months. In July 2010, 133 DM patients (=7 x 19) patients were randomly selected among 393 DM in the sampling frame; 2c) Biomedical parameters and a questionnaire are used to re-assess these patients to measure medical progress, the patient’s self-management knowledge and –skills, to ask their feedback on the intervention, on their PE, health expenditure and on medical services. 2d) To ensure independency a network of Peer Educators from outside the province is paid to carry out the re-assessment.
Methods 2 3) To calculate the ability of the intervention to recover its own cost : • Use NGO figures related to the first rural district: • Time Period: 01-10-2010 until 31-03-2011 • Total financial revenues divided by total cost for the intervention in % • Total revenues = monthly payments by contracted pharmacies to NGO for purchases of medicines delivered monthly by the NGO. • Total cost is expenses made by the NGO to purchase, import and supply the medication to the contracted pharmacies PLUS the costs of maintaining the Peer Educator Network (incentives and payments) PLUS organize all the medical services (medical consultations, laboratory and RDF) in the same period PLUS 3% of all NGO’s operational costs.
Results 1 • Early Diagnosis: The STEP Survey of 2010 found 2.3% of rural adults > 25 years old but not older than 65 years (39% of total population) with DM. Among the district population of 140,150 residents (2011) this results in an estimated prevalence of 1249 DM. Per 2011, 749 DM are registered so 60% of the estimated prevalence. Use by DM patients for self-testing fails therefore in 40% of cases to result in registration as member. The reasons for this may be multiple and not always technical. The start of active detection (mid 2007) marks the beginning of a sharp urge in awareness of DM diagnosis that lasts until 2010. Men and women benefit equally.
Results 2 Total cost of detection activities: • 2. Outcomes of July 2010 re-assessment of members with DM : • Blood Glucose: Fasting Blood Glucose (FBG) per July 2010 in the randomly selected sample (only 114 DM patients) was 145 mg/dl (=8.0mmol) on average. This is significantly lower than the average baseline value of 191 mg/dl (10.6 mmol) of the random sample. 48% of the random sample of DM patients showed FBG of ≤126 mg/dl (7 mmol).
Proportions of DM with blood pressure < 130/80 mm Hg 60% 50% 40% 30% 20% 10% 0% Baseline (since registered) Assessed per July 2010 42% 50% systolic <130 mm Hg diastolic <80 mm Hg 32% 52% Results 2 • Blood Pressure: In the same sample, the proportion of DM patients with controlled systolic blood pressure (<130 mm Hg) had increased from 42% in the baseline to 50%; whereas controlled diastolic pressure (<80 mm Hg) had increased from 32% at baseline to 52%.
Results 3 • BMI: • The proportion of DM patients with normal BMI values (18.5–23.0) improved from 36% to 41%. • Reported Health Status and feedback: • 81% of DM patients reported that they felt better than before registration and >90% reported that they were satisfied with their peer educator. • Health Expenditure: • The average reported health expenditure among the re-assessed DM patients in local currency (Riel) was equivalent to USD 3.69 per month. This is 7.1% of average rural per capita expenditure (Socio Economic Survey 2009 found USD 52 per capita per month in rural Cambodia). • Medical Consultation: • Female DM and male DM patients used medical • consultation 3.4 times in 2010, proportionately • to their sex ratio as members.
Results 4 3. Cost recovery & Sustainability Improving adherence to routine medication generates revenue to pay the continuum of care. With monthly sales at USD 566, revenue already covers the costs of Drugs, Medical Materials, Materials for Testing but not yet the Peer Educator Network, the local manager’s salary and NGO management costs. HBP patients were only registered in year 3 and have barely begun to buy medication. The intervention has been replicated to 6 other rural districts.
Conclusions & Recommendations • In Cambodia, despite few resources, a PEN can deliver secondary prevention services including access to routine medication for DM and HBP patients. • Three years onwards, the PEN performs a range of effective secondary prevention measures for DM and HBP patients at such low cost that adherence is affordable to many of its members. • If adherence by DM and in particular by HBP patients improves, the service revenue can cover the running costs of a continuum of care in rural primary care settings. • The main lesson for other low income countries is that a structured membership of chronic NCD patients can create and maintain a matching demand for and supply of health services including medicines, making the rural health system more complete and responsive and bringing universal coverage closer in view of growing health needs from chronic NCD. • With subsidy the poorest patients facing the highest monthly prescription costs can be assisted. • With subsidy the model can be more rapidly scaled-up to a point where costs and revenue break even.