Download
1 / 21
210 likes | 345 Views
Health Inequalities in the Homeless. An outreach model of healthcare delivery for homeless people in Dundee. What is homelessness?. No accommodation. At risk of domestic violence Involuntary sharing. Roofless Overcrowded Temporary accommodation

E N D
Health Inequalities in the Homeless An outreach model of healthcare delivery for homeless people in Dundee
What is homelessness? No accommodation At risk of domestic violence Involuntary sharing Roofless Overcrowded Temporary accommodation B&B Institution Emergency accommodation
Homeless presentations: Dundee 2000 - 2007 Source: Dundee City Council
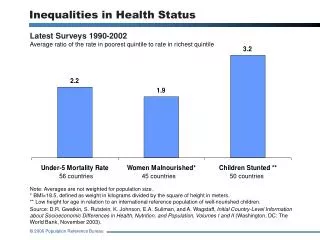
Not just a housing problem: Needs assessment 2004 • High rates of physical illness; chronic disease; mental health problems • Poor nutrition; poor oral health; smoking; alcohol; drug misuse • Adverse life-events • Difficulty accessing services; poor staff attitudes
Service needs of homeless people “Homeless people need workers to see them where they are, especially if you are moved on like me” (Male age 56)
Multidisciplinary Project Team Project lead (public health practitioner) Specialist staff - health visitor; mental health nurse Nursing staff; healthcare assistant General practitioner (1 day) Project administrator
A proactive preventive outreach model • To improveaccess to health and social care services and increase uptake of mainstream health services • Earlier detection; intervention; and treatment • Improve health outcomes; promote informed life-style choices • Inter-agency and partnership working
Reaching the target population Informal attendance at hostels Drop-in clinics One-to-one contacts Agency referrals Self-referrals
Pilot study assignment People living in homeless accommodation in Dundee City • Intervention Group • Lily Walker Centre • Salvation Army • Women’s Aid • NCH • Soapwork Lane Control Group Remaining homeless accommodation sites and other locations (Standard service: specialist health visitor)
Place of contact (N=751) Other =hospital units (acute, psychiatric, palliative care), substance misuse services
Was unmet need identified? • Complexity of unmet needs • High prevalence of learning disability, mental illness, substance misuse, physical health problems • Difficulties accessing health and related services • Levels of stigma, discrimination and institutionalisation
Evaluation question Are homeless people more likely to access health and social care services if a proactive outreach model of healthcare is used?
Post intervention follow up • 53 intervention; 42 control 4-18 months • Increased service use in both groups • Intervention group significantly higher access to drug services and open access drop-in • Increased contact with primary care services and significant increase in social work contact
Evaluation question What elements of the intervention package are responsible for changes in service usage among homeless people?
Feedback “It is difficult to register with the doctor and it is difficult to find out where to go. I mean there is no one place you can go that knows everything - everything is in its own little department and cut off from everywhere else. The social work is in one department and the mental health team in another” (Homeless person)
Feedback “They also make you feel like you deserve the help - feel like a human being -they make you feel welcome” (Homeless person )
Views of homeless service providers • The team facilitated access to care and support services • Service providers lacked knowledge and skills to respond appropriately on health-related issues • Identified gaps in services for particular groups or from certain health services • Lack of response from health services • Statutory services can feel intimidated when dealing with homeless people
Recommendations • Commitment to provide sustainable long term funding to extend and develop this service • Continue to develop effective referral pathways and robust links with all partner agencies • Promote organisational change within statutory and voluntary agencies • Explore alternative models of appropriate accommodation to meet the needs of the most vulnerable