Download
1 / 45
480 likes | 969 Views
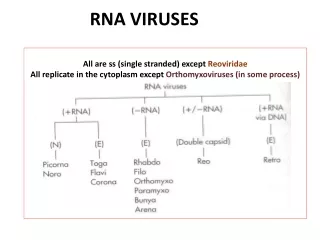
Double-Stranded RNA Viruses. Lange Chapter 40 for rotavirus, Chapter 42 for colorado tick fever SAMUEL AGUAZIM M.D. Family Reoviridae. Non-Enveloped Both double-stranded (ds) RNA and double-shelled icosahedral capsids. Segments( 10-11) Virion contains an RNA-dependent RNA polymerase.

E N D
Double-Stranded RNA Viruses Lange Chapter 40 for rotavirus, Chapter 42 for colorado tick fever SAMUEL AGUAZIM M.D
Family Reoviridae • Non-Enveloped • Both double-stranded (ds) RNA and double-shelled icosahedral capsids. Segments( 10-11) • Virion contains an RNA-dependent RNA polymerase.
Three Viruses in Family Reoviridae • Rotavirus • Orbivirus • Reovirus
Rotavirus • Major cause of infantile diarrhea worldwide • Vomiting and fever usually precede diarrhea • In healthy infants, illness lasts 3-9 days • The major serotype (A) causes diarrhea and dehydration in infants <2 years, mild diarrhea in older kids, and severe diarrhea , leading to death in malnourished individuals. • This noninflammatory diarrhea is caused by protein nsP4, a viral enterotoxin.
Family Orbivirus: Colorado tick fever virus • Transmitted by the tick Dermacentor andersoni • One of the causes of viral encephalitis • Camping and hiking in the Rocky Mountains
Family Reovirus • Asymptomatic common • May also cause a febrile disease
Hepatitis Viruses SAMUEL AGUAZIM .M.D. Lange Chapter 41
HCV- most common cause of post transfusion hepatitis most prevalent blood-borne pathogen in the U.S. • HEV: Fatality in pregnant women
Many viruses cause hepatitis. Of these, five medically important viruses are commonly described as “hepatitis viruses”: • hepatitis A virus (HAV) • hepatitis B virus (HBV) • non-A, non-B viruses, of which hepatitis C virus (HCV) is the most common • hepatitis D virus (HDV, delta agent) • Hepatitis E virus (HEV).
HEPATITIS A VIRUS Disease:HAV causes hepatitis A. Important Properties: • enterovirusclassified in the picornavirus family. • single-stranded positive polarity RNA genome • nonenveloped icosahedral nucleocapsid • replicates in the cytoplasm of the cell. • known as enterovirus 72. • one serotype • no antigenic relationship to HBV or other hepatitis viruses.
HAV Transmission & Epidemiology: • transmitted by the fecal-oralroute. • appears in the feces 2 weeks before the appearance of symptoms. • Children are the most frequently infected group • summer camps and boarding schools. • fecally contaminated water or food such as oysters grown in polluted water and eaten raw. • Unlike HBV, HAV is rarely transmitted via the blood, because the level of viremia is low • chronic infection does not occur.
Pathogenesis HAV: • probably replicates in the GI tract and spreads to the liver via the blood. Hepatocytes are infected. • infection of cultured cells produces no cytopathic effect. • likely that attack by cytotoxic T cells causes the damage to the hepatocytes. • no chronic infection occur. HAV Immune response • IgM antibody, detectable at the time jaundice appears followed 1—3 weeks later by the production of IgG antibody, which provides lifelong protection. • IgM Important in the laboratory diagnosis of hepatitis A.
HAV Clinical Findings: • Fever, anorexia (diminished appetite) nausea, vomiting, and jaundice are typical. • Dark urine, pale feces, and elevated transaminase levels are seen. • Most cases resolve spontaneously in 2—4 weeks. • short incubation period (3—4 weeks) or ( 15-40 days), in contrast to that of hepatitis B, which is 10—12 weeks. Laboratory Diagnosis: • The detection of IgM antibody is the most important test Treatment:No antiviral therapy is available.
HAV Prevention: a. Active immunizationwith a vaccine containinginactivated HAV is available. b. Passive immunizationwith immune serum globulin prior to infection or early in the incubation period can prevent or mitigate the disease. c. Observation of proper hygiene, eg, sewage disposal and hand washing after bowel movements, is of prime importance
HEPATITIS B VIRUS • hepadnavirus family. • 42-nm enveloped virion,icosahedral nucleocapsid • core containing a partially double-stranded circular DNA genome. Important antigens • surface antigen (HBsAg): protein in the envelope which is important for laboratory diagnosis and immunization. • core antigen (HBcAg): located in the core (nucleocapsid) • e antigen (HBeAg): located in the core is an important indicator of transmissibility.
HBV • Electron microscopy of a patient’s serum reveals three different types of particles: • a few 42-nm virions and many 22-nm spheres and long filaments 22 nm wide, which are composed of surface antigen. • HBV is the only human virus that produces these spheres and filaments in such large numbers in the patient’s blood.
HBV Transmission & Epidemiology: Three main modes of transmission are: • via blood • during sexual intercourse • perinatally from mother to newborn.
HBV Facts • found worldwide but is particularly prevalent in Asia. • more than 300 million people are chronically infected with HBV. • high incidence of hepatocellular carcinoma (hepatoma)in many Asian countries • Immunization against HBV in Taiwan has significantly reduced the incidence of hepatoma in children. • HBV vaccine is the first vaccine to prevent a human cancer.
HBV Pathogenesis & Immunity: • After entering the blood, the virus infects hepatocytes • viral antigens are displayed on the surface of the cells. • Cytotoxic T cells mediate an immune attack against the viral antigens • inflammation and necrosis occur. • probably the result of this cell-mediated immune injury • HBV itself does not cause a cytopathic effect. • Antigen-antibody complexes cause some of the early symptoms, eg, arthritis, and some of the complications in chronic hepatitis, eg, immune-complex glomerulonephritis, and vasculitis.
HBV Chronic Carrier • Unlike hepatitis A patients, about 5% of patients with hepatitis B become chronic carriers of HBV. • chronic carrier: someone who has HBsAg persisting in their blood for at least 6 months. • a persistent infection of the hepatocytes, which results in the prolonged presence of HBV and HBsAg in the blood. • more likely to occur when infection occurs in a newborn than in an adult, probably because a newborn’s immune system is less competent than an adult’s. • 90% of those infected as neonates become chronic carriers. • neonatal infection is associated with a high risk of hepatocellular carcinoma. • Lifelong immunity occurs after the natural infection and is mediated by humoral antibody against HBsAg
HBV Clinical Findings: • Many HBV infections are asymptomatic and are detected only by the presence of antibody to HBsAg. • mean incubation period for hepatitis B is 10—12 weeks, which is much longer than that of hepatitis A (3—4 weeks). • clinical appearance of acute hepatitis B is similar to that of hepatitis A. • However, with hepatitis B, symptoms tend to be more severe, and life-threatening hepatitis can occur. • Most chronic carriers are asymptomatic, but some have chronic active hepatitis, which can lead to cirrhosis and death.
Laboratory Diagnosis HBV: • The most important laboratory test for the detection of early HBV infection is the immunoassay for HBsAg. • HBsAg appears during the incubation period, first viral marker detected in the blood of HBV infection and is detectable in most patients during the prodrome and acute disease
HBeAg • arises during the incubation period and is present during the prodrome and early acute disease and in certain chronic carriers. • HBeAg has a high correlation with DNA polymerase activity. • presence is an important indicator of transmissibility, and, conversely • finding of HBeAb indicates low transmissibility
HBcAg • found within the nuclei of infected hepatocytes • not generally in peripheral circulation except as an integral component of Dane particle. • Anti-HBc may be the only detected serologic marker during the early convalescent phase of an HBV infection “window phase”.
HBV Treatment: • Alpha interferon is clinically useful for the treatment of chronic hepatitis B infections. • Lamivudinethat inhibit the reverse transcriptase of HIV also effective against the DNA polymerase of HBV. HBV Prevention: • involves the use of either the vaccine or hyperimmune globulin or both. (1)Thevaccine, eg, Recombivax, contains HBsAg as the immunogen. Second generation vaccine is using recombinant DNA. (2) Hepatitis B immune globulin (HBIG) contains a high titer of HBsAb because it is prepared from sera of patients who have recovered from hepatitis B.
NON-A, NON-B HEPATITIS VIRUSES • describes the cases of hepatitis for which existing serologic tests had ruled out all known viral causes. • term is not often used because the main cause of non-A, non-B hepatitis, namely, hepatitis C virus, has been identified.
HEPATITIS C VIRUS Disease:HCV causes hepatitis C. Important Properties: • enveloped virion containing a genome of single-stranded, positive-polarity RNA. • member of the flavivirus family. • no virion polymerase. • Multiple serotypes exist.
HEPATITIS C VIRUSTransmission & Epidemiology: • transmitted via blood. • most common cause of posttransfusion hepatitis. • intravenous drug user: all new HCV infections • Sexual transmission and transmission from mother to child have been difficult to document. • most prevalent blood-borne pathogen - U.S. • 4million people in the U.S. (1—2% of the population) are chronically infected with HCV. • infects hepatocytes: 30-50% of cases progress to chronic liver diseases • Alcoholism: hepatocellular carcinoma • Cancer: caused by prolonged liver damage and rapid growth rate of hepatocytes as the cells attempt to regenerate rather than by a direct oncogenic effect of HCV.
Clinical Findings HCV • acute infection with HCV is milder than infection with HBV. • Fever, anorexia, nausea, vomiting, and jaundice are common. • Dark urine, pale feces, and elevated transaminase levels are seen Laboratory Diagnosis: • detecting antibodies to HCV in an ELISA. • Blood products can now be tested for Ab to HCV.
HCV Treatment & Prevention: • A combination of alpha interferon and ribavirin is the treatment of choice for chronic hepatitis C, but it is expensive and has side effects that can limit its use. • Patients with chronic HCV infection should be advised to reduce or eliminate their consumption of alcoholic beverages to reduce the risk of hepatocellular carcinoma and cirrhosis
HEPATITIS D VIRUS (DELTA VIRUS) Disease:Hepatitis D virus (HDV) causes hepatitis D (hepatitis delta). Important Properties & Replicative Cycle: • unusual in that it is a defective virus • cannot replicate by itself because it does not have the genes for its envelope protein. • HDV can replicate only in cells also infected with HBV, because HDV uses the surface antigen of HBV (HBsAg) as its envelope protein. • HBV is therefore the helper virus for HDV.
Transmission & Epidemiology HDV: • transmitted by the same means as is HBV • sexually, by blood • perinatally. • In the United States, most HDV infections occur in intravenous drug users who share needles. • HDV infections occur worldwide with a similar distribution to that of HBV infections.
HDV Pathogenesis & Immunity: • the pathogenesis of hepatitis caused by HDV and HBV is the same • the virus-infected hepatocytes are damaged by cytotoxic T cells. • There is some evidence that delta antigen is cytopathic for hepatocytes. • IgG antibody against delta antigen is not detected for long periods after infection • uncertain whether long term immunity to HDV exists. • Because HDV can replicate only in cells also infected with HBV, hepatitis delta can occur only in a person infected with HBV. • A person can either be infected with both HDV and HBV at the same time, ie, be “coinfected,” or be previously infected with HBV and then be infected with HDV.
HDV Laboratory Diagnosis: • detecting either delta antigen or IgM antibody to delta antigen in the patient’s serum. Treatment: • Alpha interferon can mitigate some of the effects of the chronic hepatitis caused by HDV but does not eradicate the chronic carrier state Prevention of HBV infection: • Vaccine • hyperimmune globulin
HEPATITIS E VIRUS • major cause of enterically transmitted hepatitis. • common cause of water-borne epidemics of hepatitis in Asia, Africa, India, and Mexico • uncommon in the United States. • nonenveloped, single-stranded RNA virus tentatively classified as a member of the calicivirus family. • Clinically the disease resembleshepatitis A, with the exception of a high mortality rate in pregnant women. • Pregnant women who acquire HEV have a 20% fatality rate (compared to 0.5% for the rest of the population). • India, a country where HEV is endemic.
HEPATITIS G VIRUS • member of the flavivirus family, as is HCV. • unlike HCV, which is clearly the cause of both acute hepatitis and chronic active hepatitis and predisposes to hepatocellular carcinoma, HGV has not been documented to cause any of these clinical findings.