Download
1 / 23
330 likes | 1k Views
Chapter 6 Pulmonary Embolism. Topics. Pulmonary embolism Pulmonary circulation Pulmonary vascular resistance Hypoxic pulm vasoconstriction Surface tension Surfactant. Case Study #6: Fiona. 35 yr old Ballet dancer Well until 1 week ago Central abdominal pain, nausea, vomiting

E N D
Topics • Pulmonary embolism • Pulmonary circulation • Pulmonary vascular resistance • Hypoxic pulm vasoconstriction • Surface tension • Surfactant
Case Study #6: Fiona • 35 yr old Ballet dancer • Well until 1 week ago • Central abdominal pain, nausea, vomiting • Pain shifted to right lower quadrant • Acute appendicitis • Operation, recovery seemed to be going well • 2cd day, sudden stabbing pain over L chest, dsypnea; blood-streaked sputum • Non-smoker, taking oral contraceptives for 10 yrs
Physical exam #6: Fiona • Anxious and SOB • Pain in L mid-axillary line, 5th intercostal space • No pallor, temp normal, BP normal, pulse elevated (105 bpm) • No neck vein engorgement • Pleural friction rub • No dependent edema • Right calf tenderness
Investigations • Blood chemistry normal • Po2 (78 mmHg); low • Pco2= 38 mmHg; pH=7.41 • Lung scan (radioactive albumin): absent blood flow • Lung scan (radioactive Xenon): normal • Pulmonary embolism • Treatment: Heparin, anti-coagulant therapy (Warfarin)
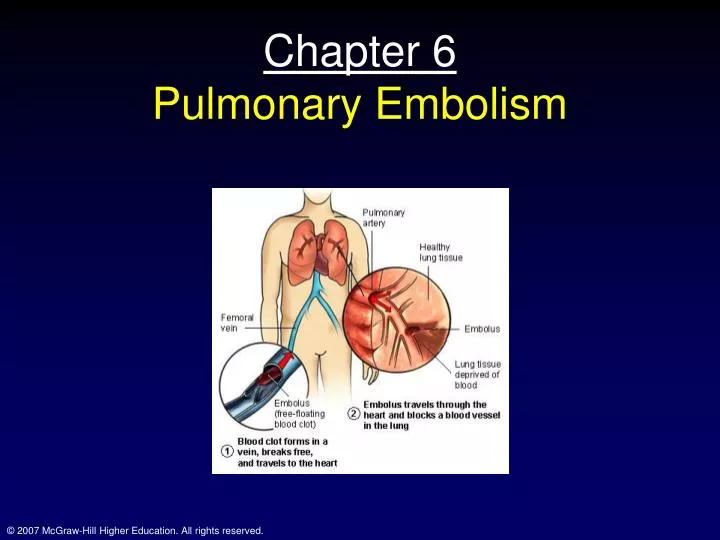
Pathogenesis • Pulmonary embolism • Frequent and potentially dangerous • Post-operation pulmonary disease • Always suspect PE • Pleural pain, blood tinged sputum, dyspnea • Combined w/ pleural friction rub, accentuated 2cd heart sound and pain and tenderness in the calf almost certain
Pathogenesis • Most commonly, emboli arise as venous thrombi from the extremities • Predisposing factors • Stasis of blood • Immobilization • Altered blood coagulation • Recent trauma and oral contraceptives • Abnormalities of vessel wall • Local trauma and inflammation • Emboli • Large emboli • Hemodynamic collapse; death in 30% of cases • Medium sized • Fiona • Small • Frequently unrecognized
Physiology and Pathophysiology of the lung • Normally, low pressure system • PVR = (Pin-Pout)/Q • PVR = (Ppa-RAP)/Q • PVR = (12-4)/6 = 1.3 mmHg/L/min • Systemic VR = • (MAP-LAP)/Q • (93-2)/6 = 15.2
Physiology and Pathophysiology of the lung • If embolus blocks lobar blood flow • PVR rises • Less than expected though • Note that an increase in either arterial or venous pressure reduces PVR; why? • Capillary distension and recruitment
Physiology and Pathophysiology of the lung • Lung volume • Also a determinant of PVR • Extra-alveolar vessels • Pulled open as lung expands • At very high lung volumes, capillaries become stretched and diameter is reduced • At low lung volumes, caps return to smaller diameter (at very low volumes, no flow)
Distribution of pulmonary blood flow • Radioactive Xenon: injected into a peripheral vein • Reaches lung units, it diffuses out (poorly soluble) • Subject holds breath and radioactivity counters determine xenon (and thus) blood flow distribution • Almost linear top to bottom increase in flow • These diffs are greatly reduced with exercise; why?
Distribution of pulmonary blood flow • About a 30 cm H2O (23 mmHg) • In zone 1: Alveolar pressure is greater than either local pulm arterial or pulm venous pressure; no flow (does not normally happen; usu. Happens with hemmorhage or Positive pressure breathing • In zone 2: Ppa>Palv>Ppv; Blood flow now determined by the diff betw. Ppa and Palv
Distribution of pulmonary blood flow • Zone 2: Starling resistor; Ppa increases down zone 2 and Palv stays the same, so flow increases down zone 2; also called “vascular waterfall” • Zone 3: Ppa>Ppv>Palv; flow determined by arterial-venous pressure drop • Blood flow increases down zone 3 as a consequence of capillary distension • Zone 4: area(s) of lung that get reduced blood flow as a consequence of low lung volume (starts at the base)
Active control of the circulation • Hypoxic pulmonary vasoconstriction • Note how blood flow falls with alveolar Po2 • Caused by low inspired Po2 and NOT by reduced PaO2 • Local phenomenon; occurs in excised lung • Note the nature of the response; suggests that lung is somewhat constricted all the time
Active control of the circulation • Hypoxic pulmonary vasoconstriction • Mechanism not fully understood • Potential factors • Increased intracellular Ca2+ (volt-gated K+ channels) • Nitric oxide • Causes smooth muscle relaxation; antagonizes HPV • Endothelin • Potent vasoconstrictors • HPV can be good • Directs blood flow away from hypoxic regions of lung (improved VA/Q) • Keeps fetal pulmonary circulation mostly closed until birth
Metabolic functions of pulmonary circulation • Angiotensin I to Angiotensin II (VC) conversion • ACE-located in pulmonary endothelium • Bradykinin: vasodilatory substance inactivated in lung by ACE • Serotonin: neurotransmitter, inactivated via uptake • Prostaglandins: vasoactive Arachidonic acid metabolites; inactivated in lung • Norepinephrine: partially taken up in lung • Leukotrienes: arachidonic acid metabolites; almost completely removed
Metabolic functions of pulmonary circulation • Arachidonic acid metabolites • Lipoxygenase and cyclooxygenase pathways • Leukotrienes • cause inflammation and bronchoconstriction • Prostaglandins • Vasoactive • Platelet aggregation • Maybe bronchoconstriction
Surface tension Surface tension: Force acting on a layer of liquid that gives it the property of an elastic sheet this is why bugs can walk on water Ex of rubber sheet and suture Blow up a bubble: surfaces of bubble contract forming a sphere (smallest surface area for a given volume); generates a pressure • Pulmonary embolism can be complicated • Alveolar hemorrhage and atelectasis • Atelectasis • Collapse • Caused by loss of surfactant and increased surface tension
Surface tension • Pressure is determined by the law of Laplace • P=4T/r • Thus, Pressure will fall as the radius of the sphere increases • Thus, a smaller sphere should empty into a larger sphere
Surface tension • Note that air inflation curve is right shifted • Reduced compliance • Due to surface tension • Surfactant • Reduces surface tension • Produced by type II alveolar cells • Contains a phospholipid; dipalmitoyl phosphatidylcholine (DPPC) • May be important contributor to respiratory distress syndrome in newborns
Surface tension • Main points • Water has very high surface tension • Placing detergent in water reduces surface tension • Lung extracts have variable surface tension • How/Why does surfactant work? • DPPC molecules are hydrophobic at one end and hydrophilic at the other; thus the individual molecules tend to repel each other, an effect that gets stronger as they get closer
Physiological advantages of surfactant • Low surface tension increases compliance • Stability of alveoli is improved (remember the tendency of small bubbles to empty into larger ones) • Surfactant reduces surface tension more in smaller bubbles • Keeps alveoli dry; elevated surface tension tends to suck fluids out of the low pressure caps
Other physiological changes with Pulmonary Embolism • Gas Exchange • Reduced Po2 • Atelectatic areas act as shunt • Pulmonary edema • Lung mechanics • Post-embolism areas receive no blood flow • Causes bronchoconstriction (reason why X-ray showed no ventilation in the region distal to emboli); short-lived usu.






















