Download
1 / 26
310 likes | 554 Views
Myocardial Viability in Ischemic Heart DZ: Assessment before Revascularization Intervention. By: Ri 黃彥霖. Outline. Introduction and definitions Imaging Techniques Conclusions. Introduction. Coronary heart dz. LV dysfunction heart failure death

E N D
Myocardial Viability in Ischemic Heart DZ:Assessment before Revascularization Intervention By: Ri黃彥霖
Outline • Introduction and definitions • Imaging Techniques • Conclusions
Introduction • Coronary heart dz. LV dysfunction heart failure death • Important determinant of prognosis: • LV function & LV myocardial viability • Outcome of medical tx remains poor • Revascularization intervention: • PCI or CABG • A promising treatment • Risk & perioperative mortality VS. Benefits
Introduction • In the last 2 decades, improvements in the use of imaging techniques to detect and assess myocardial viability, metabolism, perfusion, and function has made assessment before intervention possible
Definitions • Viable myocardium • Myocardial cells that are simply “alive” • No regard to functions, no clinical implications • Stunned myocardium • Temporary contractile dysfunction of viable myocardium caused by a brief period of ischemia followed by restoration of perfusion • Proposed hypothesis for temporary dysfunction • Oxyradical hypothesis & Calcium hypothesis • Lasts from an hour to days • Function ultimately returns to normal with normal perfusion
Definitions • Hibernating myocardium • Contractile dysfunction due to chronic reduced blood flow • Partially or completely recovery function after revascularization • Scarred/Infarcted myocardium • Nonviable myocardium with no remaining myocytes • Irreversible damage, will not recover even after reperfusion To attain the maximal benefits with minimal risk in patients with ischemic heart dz, determination of myocardial viability is important
Angiography • Earliest imaging for assessment of ventricular function and coronary artery patency • Preoperative coronary angiography and contrast ventriculography • Important indicators of prognosis • Determine causal relationship between ventricular dysfunction and coronary anatomy • Determination between PCI or CABG • Noninvasive imaging techniques are now becoming more popular
Echocardiography • Function & Viability • Detect LV wall motion defects • Performed at rest and immediately after stress • Stress methods • Exercise: treadmill or bicycle • Bruce, Cornell, Naughton protocols • Pharmacological: dobutamine • Low dose 5~10μg/kg/min increase to higher dose every 3 minutes
Echocardiography • Increase in systolic contraction at low dose dobutamine presence of viable myocardium • New regional wall motion defects, decline in EF, increase in end-systolic volume with stress myocardial ischemia
SPECT • Perfusion & Viability • Evaluate myocardial regional radioisotope uptake and regional blood flow in response to stress • Stress: blood flow up to 5x • Exercise • Pharmacological: adenosine or dipyridamole
Thallium-201 SPECT • Potassium analogue, uptake by viable cells • The degree of uptake is related directly to the coronary blood flow • “Redistribution” • Region of ischemia initially appears as area of reduced uptake apparently normal over time • Region of infarction no redistribution on delayed image. • Redistribution protocols • Stress-4 hr redistribution protocol • Late-redistribution protocol (18 to 24 hrs) • Reinjection protocol • Rest-redistribution
Technetium-99m SPECT • Similar to Thallium-201, uptake by viable cells • Higher photon energy & shorter half-life, lower radiation, allowing larger dose of injection higher quality scan with fewer artifacts • Three Tc-labeled agents: sestamibi (most frequent) teboroxime tetrofosmin
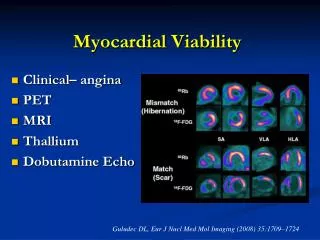
PET • Myocardial perfusion Nitrogen-13 ammonia, oxygen-15 water, rubidium-82 • Myocardial Metabolism fluorine-18 deoxyglucose(FDG) (detection and quantification of exogenous glucose utilization) • Regarded as the gold standard for assessment of myocardial viability, but clinical application is limited due to the lack of cyclotron for production of radiopharmaceuticals
PET Metabolism Perfusion
MRI • Myocardial perfusion: • Inject contrast and continuously scanning the heart • Relative perfusion deficits in regions of low signal intensity • Myocardial viability: • Inject extracellular paramagnetic contrast agent: Gadolinium-DTPA • The proposed mechanism: contrast collection in interstitial edema associated with cell necrosis and capillary plugging • Imaging 10 to 20 min after contrast injection • Late enhancement regions of myocardial necrosis and irreversible injury • No late enhancementviable
Radionuclide Angioventriculography • Assessment of ventricular function • Recording the movement of a bolus radionuclide (usually Tc-99m) during the first pass through the central circulation • Often used for the assessment of ventricular function before and after revascularization
Prognosis • How much hibernating myocardium must be present for an improvement in LVEF after revascularization to become evident? Studies ranging from 8% to 53% with a mean of 22%.
Prognosis Most studies considered LVEF of 5% as significant
Prognosis Hib = hibernation Rev = revascularization Med = medical treatment
References • “Imaging Techniques for the Assessment of Myocardial Hibernation”, European Heart Journal, 2004 (25), 815-836 • “Noninvasive Imaging of Myocardial Viability: Current Techniques and Future Developments”, Circulation Research 2003 (93), 1146-1158 • “Role of Myocardial Perfusion Imaging for Risk Stratification in Suspected or Known Coronary Artery Disease”, Heart 2003 (89), 1291-1297 • Harrison’s Principle of Internal Medicine, Ch. 211 & Ch. 226