Download
1 / 51
530 likes | 634 Views
Applied Interpretation of Clinical Studies. Jim Hoehns, Pharm.D ., BCPS, FCCP. Why is this Lecture Important?. To make informed drug therapy decisions we…. Need to understand size of treatment effect Need to relate drug information accurately

E N D
Applied Interpretation of Clinical Studies Jim Hoehns, Pharm.D., BCPS, FCCP
Why is this Lecture Important? • To make informed drug therapy decisions we…. • Need to understand size of treatment effect • Need to relate drug information accurately • Patient and physician perception of drug therapy effect influences subsequent behaviors and actions Ann Intern Med 2007;146:848-56.
Let’s Talk About “Risk”… Cohen JT. Health Aff 2007;25:636-46.
Outline • Absolute risk • Absolute risk reduction (ARR) • Relative risk (RR) • Relative risk reduction (RRR) • Odds ratio (OR) • Hazard ratio (HR) • Number needed to treat (NNT) • Number need to treat to harm (NNT:H) • aka NNH • Confidence intervals (CI)
Taking the right “STEPS” when evaluating new information S = Safety T = Tolerability “Pooled drop-out rates” E = Effectiveness -- Studies showing that the new drug is better than your current choice P = Price S = Simplicity of use Allen Shaughnessey, Pharm.D.
Point Estimation • Definition: A “point estimate” is a one-number summary of data • If you had just one number to summarize the inference from your study… • Examples: • Safety and efficacy trials: response rate, median survivals • Comparative trials: odds ratio, hazard ratio Elizabeth S. Garrett, Ph.D.
Which Looks Better? • Lipitor 80mg/d (vs. Lipitor 10mg/d) lowered the risk of MI and stroke by 22% • Lipitor 80mg/d (vs. Lipitor 10mg/d) lowered the risk of MI and stroke by 2.2%
Absolute Risk & Absolute Risk Reduction • Risk is the probability or frequency of an outcome • Migraine medication (6 mon.) • Placebo: 30% recurrence • Control event rate (CER) • Drug M: 5% recurrence • Experimental event rate (EER) • Absolute risk reduction (ARR) • CER – EER = ARR • 30% - 5% = 25%
Absolute Risk Reduction • Helps discriminate huge treatment effects from small ones • Preserves information on the baseline risk • Clinically meaningful information
Relative Risk and Relative Risk Reduction • Relative Risk - risk in treatment group relative to that in control group • Ratio of two incidence rates • EER/CER = RR • .05/.30 = 0.17 • Appropriate for trials; not appropriate for case-control studies • Relative risk reduction • Expression of reduction in relative risk • 1 – RR = RRR (1 - 0.17 = 0.83 or 83% RRR) • RRR does not tell about size of effect on an absolute scale
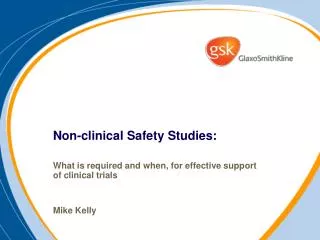
Risk of the outcome if the risk factor is present Risk of the outcome if the risk factor is absent Relative Risk Relative Risk = Example: Breast CA No Breast CA Estrogen Tx: a = 80 b = 920 a a + b Relative Risk = = 8 c c + d c = 10 d = 990 No Estrogen Tx: Measures risk of developing condition over a specified time
Odds Ratio • Retrospective study (classically) • A method of representing probability • Estimates the odds of having the RF if the condition is present divided by the odds of having the RF if the condition is not present • OR > 1: increased risk of group 1 to 2 • OR = 1: no difference in risk of group 1 compared to group 2 • OR < 1: lower risk “protective” in risk of group 1 compared to group 2
Odds of being on HRT if Breast CA present Odds of being on HRT if Breast CA not present Odds Ratio Odds Ratio = Example: Breast CA No Breast CA Estrogen Tx: a = 80 b = 920 OR = a / c = 8.6 b / d c = 10 d = 990 No Estrogen Tx:
Ross et al. • Case-control study in Los Angeles • 1897 cases with incident breast CA • 1637 controls • matched on age, race-ethnicity, neighborhood • All patients: no hysterectomy • Adjusted for breast CA risks • e.g. age at menopause, age at menarche, family Hx, nulliparity, body weight, etc. Ross et al. JNCI 2000;92:328-32.
Ross et al, Results Odds Ratio of Breast CA per 5 Years of Use
Relative Risk vs. Odds Ratio Thrombophilia Tripepi G. Kidney International 2007
Number Needed to Treat (NNT) • NNT is the number of patients needed to treat to prevent one event or outcome • reciprocal of the absolute risk reduction • E.g. 0.30 – 0.05 = 0.25 = ARR • 1/ARR = 1/0.25 = 4 = NNT • incorporates baseline risk w/o treatment and risk reduction with treatment • clinically useful; tells how much effort required to prevent one event
Number Needed to Treat • Be cognizant of the “time” factor • The smaller the NNT, the more impressive the result • Patients may have a different baseline risk than the “average” study patient • Limitations • Expressed as single number (point estimate) • “True” NNT may be higher or lower • 95% confidence intervals are useful • NNT is 7 (95%CI 3 – 11) • Need a binary outcome
Number Needed to Harm (NNH) or (NNT:H) • Number needed to treat to cause harm to one more patient • 1/absolute risk increase • Example • Adverse event (>3X ULN AST or ALT) • Lipitor 10mg QD: 0.2% • Lipitor 80mg QD: 1.2% • 1/0.01 = 100 NNH
Putting it Together McQuay, H. J. et. al. Ann Intern Med 1997;126:712-720
Don’t Forget….. • Relative risk reduction is always larger, and “looks” better than absolute risk reduction
Confidence Intervals (CI) • Provides a measure of precision (or uncertainty) of an estimate (i.e.study results) for making inferences about the population of all such patients • 95% CI • 95% of such intervals will contain the true population value • Range of values within which we can be 95% sure that the true value lies • The smaller the study (i.e. less patients) the wider the confidence intervals
Confidence Intervals • CIs and significance tests are closely related mathematically • A “significant” P value of <0.05 will correspond to a 95% CI which excludes the value indicating no difference • 0 for the difference between 2 means or proportions • 1 for a relative risk or odds ratio
Which of the following lipid parameters were significantly changed in patients receiving the soy-containing diets?
Which quartile group is significantly different from the <30 group?
HRT and Breast Cancer Nurses Health Study, 1978 to 1992 NEJM 1995;332:1589-93.
Hazard Ratio • Compares the risk of event in two populations • A relative measure • Ratio of risk in group 1 to risk in group 2 • Assumption: “proportional hazards” • “risk is constant over time” • Used to analyze time-to-event curves
WHI Study Summaries Hazard Ratio (95% CI) JAMA 2004;291:1769-71.
Intensive Lipid Lowering – Acute Coronary Syndromes • PROVE IT-TIMI 22 Study • Treatment: Pravachol 40mg QD (LDL goal <100) vs. Lipitor 80mg QD (LDL goal~70) • Statin naïve (75%): baseline TChol ≤240 • On statins (25%): baseline TChol ≤200 • N=4,162 with ACS in past 10 days • Mean duration: 2 years • Primary outcome: death (any cause), MI, unstable angina, PTCI, or CABG N Engl J Med 2004;350:1495-504.
PROVE IT - Results • Mean LDL • Pravachol 40mg: 106 (baseline) 95mg/dL • Lipitor 80mg: 106 (baseline) 62mg/dL • Primary outcome • Pravachol 40mg: 26.3% • Lipitor 80mg: 22.4% • Baseline LDL ≥125mg/dL: 34% RRR • Baseline LDL <125m/dL: 7% RRR • Safety • >3XULN ALT: Pravachol 40mg: 1.1%, Lipitor 80mg 3.3% • DC med due to myalgias/CK: Pravachol 2.7%, Lipitor 3.3% • DC rate: Pravachol (33%), Lipitor (30.4%) RRR 16% ARR 3.9% NNT 25.6 P=0.02 N Engl J Med 2004;350:1495-504.
Intensive Lipid Lowering in Patients with Stable Coronary Disease • TNT Study • Treatment: Lipitor 10mg QD (LDL goal <100) vs. Lipitor 80mg QD (LDL goal: 75 mg/dL) • 8 week run-in of Lipitor 10mg QD • Randomized if LDL <130 • N=10,001, median duration: 4.9 yrs • History of MI, angina, and hx of revascularization • Primary endpoint: CHD death, MI, resuscitation after cardiac arrest, or stroke N Engl J Med 2005;352:1425-35.
TNT Study - Results • Mean LDL • Lipitor 10mg: 98mg/dL (baseline) → 101mg/dL • Lipitor 80mg: 97mg/dL (baseline) → 77mg/dL • Primary outcome • Lipitor 10mg: 10.9% • Lipitor 80mg: 8.7% • Mortality • All-cause: HR 1.01 (0.85-1.19) • Noncardiovascular: • Lipitor 10mg (2.5%), Lipitor 80mg (3.2%) HR: 1.25 (0.99-1.57) P=0.06 RRR 22% ARR 2.2% NNT 45
TNT – Cost Analysis • Drug cost • 10mg (1yr) $811; 10mg (4.9yrs) $3,974 • 80mg (1yr) $1,119; 80mg (4.9yrs) $5,484 • NNT = 45.4 • 45.4 X $5,484 = $248,980 • Incremental cost over 10mg QD • $248,980 - $180,420 = $68,560 www.drugstore.com Aug 2005
CLASS Study • Annualized incidence of upper GI ulcer complications • Celecoxib 0.76% • NSAIDs 1.45% • Relative risk 0.53 (0.26-1.11) • Absolute risk reduction 0.69% • NNT= 145
CLASS Study • Annualized incidence of upper GI ulcer complications plus symptomatic ulcers • Celecoxib 2.08% • NSAIDs 3.54% • Relative risk 0.59 (0.38-0.94) • Absolute risk reduction 1.46% • NNT= 68.5 • Cost of preventing one event= $49,715
Summary • Distinguish between absolute and relative (benefits or harms) drug effects • RRR looks “better” than ARR • NNT is a useful measure • Relative measures • Odds ratio, relative risk, hazard ratio • <1: “protective” effect; lower risk • 1: no difference in risk • >1: increased risk
For the 3 abstracts determine….. • ARR • NNT • RR • RRR
NNT 5.0 (4.1-6.9) NNT 3.1 (2.6-3.8) Pain 1997;70:193-201
A B Clinically significant?? C D
Study B (Hypertension) • Fatal or nonfatal stroke • Placebo (CER): 17.7% • Indapamide (EER) 12.4% • ARR: 17.7 – 12.4 = 5.3% • NNT = 1/0.053 = 18.9 or 19 (over 18 mon.) • Relative risk: .124/.177 = 0.7 • Reported HR: 0.7 (0.49 – 1.01) • RRR: 1 – 0.7 = 0.3 or 30%
Study C (diabetes) • Nonfatal MI, nonfatal stroke, or CV death • Standard tx (CER): 7.2% • Intensive tx (EER): 6.9% • ARR: 7.2 – 6.9 = 0.3% • NNT: 1/0.003 = 333 • Relative risk: 0.069/0.072 = 0.96 • RRR: 1 – 0.96 = .04 or 4% • Statistically nonsignificant result