Download
1 / 37
380 likes | 561 Views
Tutorial – Gaseous Exchange. Gaseous Exchange. General factors affecting ‘flow’ F = k * Δ P / R K = constant Δ P = delta P, ‘pressure gradient’ R = ‘resistance’ For exchange of respiratory gases in lungs… R is related to cross-sectional area and thickness

E N D
Gaseous Exchange • General factors affecting ‘flow’ • F = k * ΔP / R • K = constant • ΔP = delta P, ‘pressure gradient’ • R = ‘resistance’ • For exchange of respiratory gases in lungs… • R is related to cross-sectional area and thickness • K is related gas under consideration • Molecular weight • ‘velocity’ • Solubility
Gaseous Exchange • D = (A * ΔP * s) / (d * sqrt(MW) ) • D = diffusion rate • A = diffusion area • ΔP = partial pressure difference • s = solubility • d = diffusion distance • MW = molecular weight
Gaseous Exchange • Partial pressure • Pressure exerted by individual gas, independent of others • O2 = 20.93 % • If P = 760 mmHg, PO2 = 20.93/100 * 760 = 159 mmHg • Gas diffuses down a partial pressure gradient • When no gradient, no net (nett) movement • Gas can diffuse into water • By definition, when air/liquid in equilibrium (ie equal diffusion in and out), the partial pressures are the same • When partial pressures differ, the gas will move down its partial pressure gradient • Partial pressure should not be confused with concentration • Conc a function of both partial pressure & ‘solubility’
Gaseous Exchange • A = 50 square metres • over which ~ 100 ml blood is ‘smeared’ – a monolayer! • d = down to 0.5 microns • Diffusing capacity of respiratory membrane… • Oxygen ~ 21 ml / min / mmHg • Normal pressure gradient is 11 mmHg 230 ml/min at rest • Carbon dioxide • Difficult to measure but >400 ml / min / mmHg • Can increase diffusing capacity by… • Increasing perfusion of under-perfused parts of lungs • Increasing CO (blood normally equilibrates 1/3rd along cap)
Gaseous Exchange • Some parts of lungs very poorly perfused at rest • Do not need that capacity, can exchange all the gases we need over a smaller area • Link between ventilation (V) and perfusion (Q) • V/Q (or V/P) ratio • Approx 0.85 • Large V/Q means more air ventilated than needed to service the blood flowing through the lungs • Wasted ventilation • Low V/Q means more blood flowing than needed • Incomplete oxygenation, so wasted cardiac output • Called a ‘physiologic shunt’ (as if part of CO not put through lungs)
Gaseous Exchange • ‘Ventilation’ of respiratory membrane a bit of a myth • As airways divide, each gets smaller… • But cross-sectional area gets greater • Thus, velocity of air gets smaller the further down the respiratory ‘tree’ • ‘Bulk flow’ approaches zero at the alveoli • Helps keep alveolar composition fairly constant and exchange with blood fairly constant in face of intermittent breathing • Significant proportion of exchange is by diffusion • Alveoli small enough that O2 in middle can diffuse • Similar to a river wide delta (eg Nile)
Obstructive Airway Diseases • Chronic (Obstructive) Bronchitis • Emphysema • Bronchiectasis • Asthma
Chronic Bronchitis & Emphysema • Almost always co-exist • Together known as Chronic Obstructive Pulmonary Disease (COPD) • or Chronic Obstructive Airway Disease (COAD) • Affects 6% of men and 4% of women over 45 in UK • Chronic bronchitis is • chronic productive cough for 3 mo per year for 2 years • Emphysema is • permanent enlargement of the airspaces distal to terminal bronchioles • a result of alveolar wall destruction
COPD: Definition • A disease state characterised by airflow limitation that is not fully reversible • compounded by effects of emphysema on gas exchange at resp membrane • Airflow limitation is usually both • progressive and • associated with abnormal inflammatory response of lungs to noxious particles or gases • primary cause is tobacco smoke
COPD: Facts • COPD is the 4th leading cause of death in the United States (behind heart disease, cancer, and cerebrovascular disease) • In 2005, the WHO estimated >3 million deaths worldwide from COPD • ~5% global deaths • ~90% in low/middle income countries • ~65 million sufferers globally • In 1990, COPD was ranked 12th as a burden of disease; by 2020 it is projected to rank 5th • Burden probably under-estimated as not usually recognised/diagnosed until moderately advanced • Global burden/cost set to increase with increase in tobacco use in developing countries, ageing population, increasing cost of medical intervention
% Change in Age-Adjusted Death Rates, US, 1965-98 Proportion of 1965 Rate 3.0 Coronary Heart Disease Stroke Other CVD COPD All Other Causes 2.5 2.0 1.5 1.0 0.5 –59% –64% –35% +163% –7% 0 1965 - 1998 1965 - 1998 1965 - 1998 1965 - 1998 1965 - 1998 Source: NHLBI/NIH/DHHS
COPD: Ethnicity Deaths per 100,000 60 50 40 30 20 10 0 1960 1965 1970 1975 1980 1985 1990 1995 2000
COPD: Smoking Fletcher C, Peto R. Br Med J, 1977.(1):1645
COPD: Mortality Trends 1990 2020 Ischemic heart disease Cerebrovascular disease Lower resp infection Diarrheal disease Perinatal disorders COPD Tuberculosis Measles Road traffic accidents Lung cancer 3rd 6th Stomach Cancer HIV Suicide Murray & Lopez. Lancet 1997
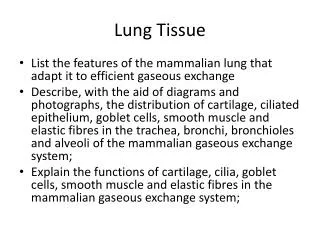
Chronic Bronchitis • Nowadays, almost always due to smoking in UK • air pollution a significant cause elsewhere • Eg; in India, use of biomass fuels circa 400-550 thousand premature deaths annually • Hypersecretion of mucous • Mucous gland hypertrophy • Loss of ciliated epithelia
Chronic Bronchitis • May also see… • squamous metaplasia of bronchial mucosa • submucosal oedema • lymphocytic infiltration • intraalveolar fibrosis • Leads to… • Inflammatory narrowing and fibrosis of bronchioles, impeding air flow • Goblet cell metaplasia leading to hypersecretion of mucous, further impeding air flow • Air sac distension and rupture (i.e. emphysema) • Decreased lung compliance (fibrosis)
Emphysema • Dilation of acinar airspace due to destruction of interalveolar septa • Due to proteolytic enzymes released from white cells during inflammation? • Common causes are smoking and air pollution • low grade chronic pulmonary inflammation • Oxidants in smoke believed to inhibit normal anti-proteolytic activity of serum globulins
Emphysema: Physiological Effects • Reduction in elasticity (compliance) of lung tissue • remodelling airway/ductal collapse during expiration • interferes with air flow to/from respiratory part of lung • Gas exchange area is also reduced • Progressive dyspnoea and hypoxaemia • Development of corpulmonale • Smaller surface area • fewer capillaries, esp ‘in parallel’ increased resistance. • Hypoxaemia vasoconstriction (reverse of other tissues) • increased pulmonary artery pressure • increased afterload on right ventricle • right heart failure
COPD: Role of Inflammation • There is a chronic inflammatory process in COPD • But, it differs markedly from that seen in asthma • different inflammatory cells, • mediators, • inflammatory effects, • responses to treatment
COPD: Inflammatory Cells/Mediators • Cigarette smoke/irritants activate macrophages and airway epithelial cells • neutrophil chemotactic factors • including interleukin-8 and leukotriene B4. • Neutrophils and macrophages release proteases • break down connective tissue in the lung parenchyma • emphysema and mucous hypersecretion. • Proteases are normally counteracted by protease inhibitors, eg • (alpha)1-antitrypsin, • secretory leukoprotease inhibitor • tissue inhibitors of matrix metalloproteinases • Cytotoxic T cells (CD8+ lymphocytes) may also be involved in the inflammatory cascade. • MCP-1 is monocyte chemotactic protein 1 • released by and affects macrophages
COPD: Protease-Antiprotease Imbalance • Proteases • Neutrophil elastase and proteinase 3 • neutrophil-derived serine proteases • Cathepsins • Can produce emphysema in laboratory animals. • Serine proteases • mucus secretion (link to chronic bronchitis?) • Antiproteases • Inhibitors of serine proteases • (alpha)1-antitrypsin in lung parenchyma • airway-epithelium-derived secretory leukoprotease inhibitor in the airways • Three Tissue Inhibitors of Matrix metalloProteinases (called TIMP-1, TIMP-2, and TIMP-3) • Elafin (skin-derived antileukoprotease– SKALP)
COPD: Protease-Antiprotease Imbalance • Balance tipped in favour of increased proteolysis • either an increase in proteases • or a deficiency of antiproteases • Balance set by noxious irritants (eg smoking) and host/genetic factors
COPD: Role of Oxidative Stress • Compounds generating oxidative stress • H2O2 hydrogen peroxide, • O2- superoxide anion, • OH• hydroxyl radical (unpaired electron), • ONOO-peroxynitrate • Lead to… • …decreased antiproteasedefences • …activation of nuclear factor-(kappa)B • increased secretion of the cytokines interleukin-8 and tumor necrosis factor (alpha) • …increased production of isoprostanes • Oxidative stress marker • …other, direct effects on airway functions
Weight loss in COPD • Increased circulating levels of leptin, which may contribute to weight loss in these patients • Increased metabolism • loss of skeletal muscle and wasting of limb muscles • Skeletal-muscle weakness is a common feature of COPD • exacerbates dyspnea • The weakness is due to a combination of chronic hypoxia, immobility, and increased metabolic rate • Profound decrease in myosin heavy chain in skeletal muscles
COPD : Archetypes • Pink Puffer vs Blue Bloater • Extremes of a spectrum • ‘End Stage’ • Medical illustrations by Dr Frank Netter in 1950s
COPD : Archetypes – The Pink Puffer • COPD Type A – Emphysema • Hyperinflation/barrel chest • Tachypnea/pursed lips • Increased V/Q • Tachypnea / Low CO • Systemic hypoxia (low CO) • Weight loss • Problems eating & breathing at same time?
COPD : Archetypes – The Blue Bloater • COPD Type B – Chronic Bronchitis • Decreased V/Q • Poor ventilation / High CO • Cyanosis • CO2 retention • Acidosis • Pulmonary arteriolar constriction • Right heart failure