Download
1 / 26
260 likes | 472 Views
TAXUS Perseus Core Data Elements: Qualitative and Quantitative Angiography. Jeffrey J. Popma, MD Alexandra Almonacid, MD Brigham and Women’s Hospital St. Elizabeth Medical Center Tufts University School of Medicine Boston, MA. Angiographic Core Laboratory.

E N D
TAXUS PerseusCore Data Elements:Qualitative and Quantitative Angiography Jeffrey J. Popma, MD Alexandra Almonacid, MD Brigham and Women’s Hospital St. Elizabeth Medical Center Tufts University School of Medicine Boston, MA AngiographicCore Laboratory
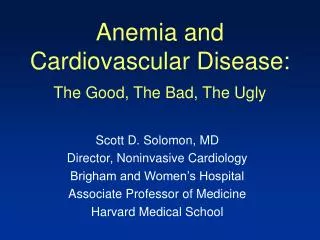
Core Lab Lessons: Beyond Late Lumen Loss • After 15 years, substantial observer variabilities are still found with qualitative angiographic interpretations independent Core Laboratory analyses have become standard for FDA DES studies • Discrepancies noted with Clinical Site Observations: • Baseline % diameter stenosis (e.g., NASCET Carotid) • Lesion Length and Reference Vessel Diameter • Final Angiographic Result • Binary restenosis (? 50-70% threshold for revascularization) • “Oculostenotic reflex”
Core Lab Lessons: Beyond Late Lumen Loss • Our initial focus with QCA was to determine the late term lumen dimensions, and relate them to the early angiographic results and late clinical events • Balloon angioplasty – less acute gain; less late loss • DCA – more acute gain; more lumen loss; better net gain • Continuous measures replaced binary criteria • Loss index (LL/AG) provided relative benefit --> drugs failed • With stents, LL was attributable to intimal hyperplasia. • Acute gains and late loss was similar (essentially) for all bare metal stents • ? Possible exception related to strut thickness • Late loss replaced loss index as a surrogate
Beyond Late Lumen Loss • Clinical indices were further refined to determine those events that directly related to failure of the stent • TLR replaced “any” revascularization and TVF (in some studies) • Early (< 30 d) stent thrombosis was not included in the criteria for “restenosis” or calculations for late lumen loss but was placed in the early clinical failure category alone • To lower sample sizes, “surrogate” markers were sought to identify was to lower sample sizes required for device approval • In-Lesion (Segment) late lumen loss became the preferred endpoint for many device trials
in-segment in-stent (all stents used to treat the target lesion) QCA methodology 5 mm 5 mm stented segment proximal edge distal edge
Angio Restenosis is any late loss over 1.5 mm (50% DS) Clinical TLR correlates with late loss over 2.1 (70% DS) Pts. with angio restenosis Pts. with clinical restenosis BMS Restenosis was Near Gaussianallowing expression with mean±SD Example: 3.0 mm Bare Metal Stent Mean late loss = 1.0 ± 0.5 mm Mean late loss 1.0 Pts. w/o restenosis 0.8 0.6 Distribution Density 0.4 0.2 0.0 -0.50 -0.25 0.00 0.25 0.50 0.75 1.00 1.25 1.50 1.75 2.00 2.25 2.50 Late loss (mm) Donald Baim, Summer in Seattle, 2006.
DES Have Different Late Loss Distributions Mean late loss = 0.2 mm Clinical restenosis What % of patients are above that line? 0.4 mm 0.6 mm 1.0 mm (BMS) Mauri et al. Circulation. 2005;111:3435
TAXUS-IV Angiographic predictors of TLR Follow-up % Diameter Stenosis is a Better Predictor ROC Analysis combining all patients 1.0 Late Loss AUC = 0.918 MLD AUC = 0.940 0.5 Sensitivity Diameter Stenosis AUC = 0.944 0.0 0.0 0.5 1.0 1 - Specificity
Surrogate Angiographic Endpoints LL and % DS vs. TLR - A curvilinear relationship 11 RCTs with Cypher, Taxus, Endeavor, and BMS (5381 pts) All patientsRVD <2.5mmRVD 2.5-3.0mmRVD > 3.0mm All patients Probability of TLR Probability of TLR In-stent late loss In-segment %DS Pocock S et al ACC 2006
Sidebranch Compromise With Overlapping StentsTAXUS V Multiple Stent Analysis Blinded core lab analysis of all multiple stent patients • Main Vessel Analysis: • Main vessel No Reflow, TIMI flow, Dissection, Distal Embolization, Abrupt Closure • Side Branch Analysis (for branches >1 mm): • Branch occlusion (total occlusion) • Branch narrowing (Δ≥70% 100%) • Branch TIMI flow
Sidebranch Occlusion Side Branch Narrowing (Δ ≥ 70% 100%) TIMI Flow Reduction Side Branch Analysis in Multiple Stenting
Control TAXUS p=0.74 p=1.00 p=0.10 p=0.025 p=0.23 p=1.00 37/203 51/203 56/203 21/48 12/48 8/48 34/207 58/207 68/207 24/55 15/55 26/55 Non-overlap region Non-overlap region Non-overlap region Overlap region Overlap region Overlap region Impact of the Overlap Region(per side branch) Any Sidebranch Occlusion Any Sidebranch Narrowing Any TIMI Flow Reduction
Definitions Used for Stent Fracture 1 Allie et al Endovascular Today 2004; July/August: 22-34 2 Scheinert et al J Am Coll Cardiol 2005; 45:312-315 * Type 5 implies spiral fracture of stent
Stent Fractures Type 4 Stent Fractures Stent Fracture with 3 mm of Stent Overlap
Incidence of TAXUS-Express Stent Fracture Detailed angiographic review of TAXUS IV and VI Core Lab remains blinded due to ongoing adjudication Taxus IV: 7 Fractures TAXUS VI: 3 Factures - Type 1 N=3 - Type 1 N=1 - Type 2 N=1 - Type 2 N=1 - Type 3 N=1 - Type 3 N=1 - Type 4 N=2 - Of the 10 fractures, 5 cases had overlapping stents (all overlaps were longer thatn 3 mm). In 4 of 5 cases, the stent fracture was within 5 mm of the overlap * Preliminary Analysis
Incidence of TAXUS Stent Fracture In patients assigned to angiographic FU 0.85% 0.81% 0.71% N=819 N=420 N=1239 Taxus IV Taxus VI Overall
Taxus IV 145-247 24.9mm Stented Segment Overlap >3mm TAXUS-Express Type I Fractures
Fundamental “Pitfalls” for the Seasoned Professional Interventionalist • Forget the angiographic inclusion and exclusion criteria, the patient really needs the Taxus Perseus stent • “I don’t really see a stenosis, but it must be tight behind that diagonal branch” or “Who needs two views, it looks pretty tight in this one” • I’m sure the Core Lab can measure that tip of the injection catheter • Who needs documentation, I’ll remember all the views I took when the patient comes back for at follow-up • I can’t believe that this lesion isn’t causing symptoms, I going to fix it anyway
Pitfalls in QCA • Make certain that all patients meet the angiographic inclusion and exclusion criteria with respect to lesion length, vessel size, and lesion complexity • A “Friendly Feedback” sheet will give you a 20 point score for the film quality • Dr. Almonacid and I will provide “personal” feedback if we disagree with the patient being enrolled in the study. Remember, we’re colleagues and friends, but . . . .
Pitfalls in QCA • An accurate calibration source (the injection catheter filled with contrast) is the only way that we can identify the absolute changes in the MLD, edges, and within the stent between the final and the follow-up • We need to see the very distal, nontapered portion of the catheter and document the size of the catheters on the Technician’s • Nitroglycerin with the final stent placement and at FU is essential to control vasomotor tone for the calculations of late lumen loss
Pitfalls in QCA • “Who needs the documentation, I will remember the views I took when the patient comes back for follow-up” Please Use the Worksheet
Pitfalls in QCA • At the time of follow-up angiography, you see and intermediate stenosis (50-60%) and say “I can’t believe that this lesion isn’t causing symptoms, I going to fix it anyway”
Summary • Core QCA data elements should include conventional morphologic and quantitative angiographic parameters in order to classify “tested” and “untested” therapies - Newer analysis methods are needed for bifurcations • Late lumen loss is a reason index (% diameter stenosis may be better) for the late angiographic outcome but its ability to predict TLR (and MACE) may be limited in DES v. DES studies • Core QCA elements should add sidebranch patency (for overlapping stents), stent fracture, aneurysms, and stent thrombosis to assess long-term safety
Technologist Worksheet or detailed catheterization report with sequential angiographic views • Dicom3 Compatible CDs or 35 mm film • Please don’t forget the nitroglycerin • Follow Image Acquisition Guidelines • Match 2 Pre, Final, and Follow-up • Document everything on cine, particularly in the radiation studies • Near 100% angiographic follow-up is essential Simple QCA Requests