Download
1 / 68
700 likes | 863 Views
General Pathology (DENF 2701) Topic: Neoplasia. Fall, 2004; Wednesdays, 10:00-12:00 am; Room 132 Course Director: Dr. Jerry Bouquot Room 3.094B; 713-500-4406; 713-520-1250 (home). Neoplasia “New Growth”; From Latin Word for Crab. Cancer: Neoplasms are not controlled by the body

E N D
General Pathology (DENF 2701)Topic: Neoplasia Fall, 2004; Wednesdays, 10:00-12:00 am; Room 132 Course Director: Dr. Jerry Bouquot Room 3.094B; 713-500-4406; 713-520-1250 (home)
Neoplasia“New Growth”; From Latin Word for Crab • Cancer: Neoplasms are not controlled by the body – Continue to replicate indefinitely – Tumors may flourish, even while the host is wasting away – Cancers induce increased blood supply • Cancer: 2nd leading cause of US deaths -- After cardiovascular disease • Oncology = study of tumors (“oncos” = tumor, “logos” = study of) -- Oncologist = physician who treats cancer exclusively – Hemoncologist = specializes in leukemias, lymphomas, etc. -- Hematologist = blood doctor, treats leukemias, lymphomas, etc. – Surgical oncologist; Radiation oncologist • Typically monoclonal • Malignant (cancers): invade, destroy, metastasize (distant spread) • Benign: nonmalignant neoplasm; add suffix “-oma”
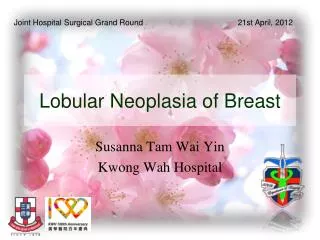
NeoplasiaBenign v. Malignant Leiomyoma Benign Smooth Muscle Neoplasm Photos: Kumar, Cotran, Robbins. Robbins Basic pathology, 7th ed., Saunders, Philadelphia, 2003; Stevens A, Lowe J. Slide atlas of pathology. Mosby, London, 1995. .
NeoplasmsBenign v. Malignant Thyroid Adenoma Breast Adenocarcinoma Breast Adenocarcinoma Photo: Stevens A, Lowe J. Slide atlas of pathology. Mosby, London, 1995.
NeoplasiaDifferentiation of Cells/Tissue • Well differentiated: cells look mature and similar to original cells -- Grade I = cells are well differentiated -- Grades II and III: moderately differentiated --Grade IV = poorly differentiated • Not very good at prognosis • Poorly differentiated: cells look immature and irregular -- Grade IV; high grade -- Often means worse prognosis • More mature or differentiated cells retain function – e.g. squamous cell carcinoma makes keratin (keratin pearls, epithelial pearls) -- e.g. mucoepidermoid carcinoma makes mucus (mucin)
NeoplasiaDifferentiation of Cells/Tissue • Anaplasia (“to form backwards”): very undifferentiated -- Primitive cells • Stem cells of some tumors undergo divergent differentiation – e.g. pleomorphic adenoma (mixed tumor) of salivary glands – e.g. fibroadenoma of breast • Certain tumors induce stromal change (not differentiation) -- Fibrosis (desmoplasia) -- New vessels (angiogenesis)
Squamous Cell CarcinomaMicroscopic Grading Grade I Grade III Grade IV Grade II
Loss of Differentiation & Maturity Well differentiated adenocarcinoma of colon Benign neoplasm of colon Photos: Stevens A, Lowe J. Slide atlas of pathology. Mosby, London, 1995.
Loss of Differentiation Anaplastic carcinoma of colon Poorly differentiated adenocarcinoma of colon Photos: Stevens A, Lowe J. Slide atlas of pathology. Mosby, London, 1995.
Signs of DysplasiaNot Necessarily Associated with Cancer • Pleomorphic (abnormal shape) -- Cells and/or nuclei • Enlargement...cells or nuclei • Reduced cytoplasmic/nuclear ratio -- Large nucleus compared to cell size -- 1:1 vs. 1:4 - 1:6 for normal • Hyperchromatic nuclei -- Chromatin is course, clumped • Increased mitotic rate -- Numerous mitotic figures • Bizarre mitoses: abnormal shape -- e.g. tripolar/quadripolar mitoses -- e.g. abnormal location
Signs of DysplasiaNot Necessarily Associated with Cancer • Lack of cohesion (detached cells) • Prominent, perhaps multiple nucleoli • Loss of polarity (no orientation) • Bizarre cells • Problem: some dysplasias are not related to cancer e.g. Developmental anomalies Bone dysplasias • Problem: not all dysplasias progress to malignancy (precancer) Photos: Stevens A, Lowe J. Slide atlas of pathology. Mosby, London, 1995; Kumar, Cotran, Robbins. Robbins Basic pathology, 7th ed., Saunders, Philadelphia, 2003.
The Dysplastic Cell Photo: J. Bouquot. Pract Perio Aesth Dent, 1995.
Extra Credit Question Melanoma is a malignancy of which of the following cells? • Fibroblast • Osteoblast • Melanocyte • Nevus cell • Smooth muscle cell
TeratomaA Type of Neoplasm as Well as Developmental Anomaly • Usually congenital • More than one germ-cell type • From multipotential cells -- Therefore usually found in ovary or testis • Usually helter-skelter mix of tissue types -- May be so mature that small “babies” develop • May be benign or malignant • Not a hamartoma (mass of disorganized tissue indigenous to the site) • Not a choristoma (congenital anomaly, a heterotopic rest of cells) • Cervical teratoma is usually fatal -- Because it presses on vessels, airways, esophagus
Pituitary TeratomaWith Teeth Photo: Dr. J. Bouquot, West Virginia University, Morgantown, West Virginia
NeoplasiaInvasion • One of two things that most clearly separate benign from cancer – Exceptions: Basal cell carcinoma (skin) Verrucous carcinoma (mouth) Prostate carcinoma -- Exceptions: Hemangioma Lymphangioma Lipoma • Not all benign neoplasms are encapsulated -- Usually a well-defined cleavage plane • After the ability to metastasize, the ability to invade is the most reliable feature of malignancy Cuniculatum (Verrucous?) Carcinoma Hemangioma Photos: P. Morgan, Guys Hospital, London, England; J. Bouquot, West Virginia University, Morgantown, West Virginia.
Carcinoma in situTop-to-Bottom Dysplasia Severe Dysplasia Photos: Kumar, Cotran, Robbins. Robbins Basic pathology, 7th ed., Saunders, Philadelphia, 2003.
Local InvasionColonic adenocarcinoma (left) invades into muscle (right) Photo: Stevens A, Lowe J. Slide atlas of pathology. Mosby, London, 1995.
NeoplasiaMetastasis • Secondary implants of cancer cells separate from 10 tumor • The most unique thing about malignancy (v. benignancy) • Carcinomas spread via lymphatics to local lymph nodes – Oral cancer: cervical enlarged, firm, fixed (perhaps matted) lymph nodes – Breast cancer (usually is in upper outer quadrant): axillary lymph node involvement (perhaps with lymphedema) – Lung cancer: bronchial lymph node involvement • Usually ipsilateral (on same side of body) node -- May be contralateral (opposite side of body) • Sarcomas spread via blood stream -- Therefore: pulmonary mets usually • Usually metastasis is from long-standing, large cancers -- There are exceptions!!
Cellular Events Needed for Metastasis Photos: Stevens A, Lowe J. Slide atlas of pathology. Mosby, London, 1995.
Local Lymphatic InvasionPara-Aortic Lymph Nodes Photo: Stevens A, Lowe J. Slide atlas of pathology. Mosby, London, 1995.
Main Routes of Tumor SpreadCarcinoma of the Lung Hilar Lymph Nodes (cancer = white deposits Photo: Stevens A, Lowe J. Slide atlas of pathology. Mosby, London, 1995.
Most Common Sites of Distant Metastasis Liver Metastases Photos: Stevens A, Lowe J. Slide atlas of pathology. Mosby, London, 1995; Kumar, Cotran, Robbins. Robbins Basic pathology, 7th ed., Saunders, Philadelphia, 2003. .
Epidemiologic Terms • Incidence rate: number of newly diagnosed cancers/year • Mortality rate: number of patients dying from cancer/year • Prevalence rate: number of cancers diagnosed in a certain population at a given point in time (point prevalence) • Relative frequency rate: proportion of all cancers represented by an individual cancer • Epidemiologic studies (case-control studies, differences in incidence between groups, etc.) are the best “proof” of etiology (cause), but they are very expensive and time-consuming
Incidence of CancerMore than 100 Different Types of Cancer Photo: Kumar, Cotran, Robbins. Robbins Basic pathology, 7th ed., Saunders, Philadelphia, 2003.
CancerAge as an Etiologic Factor • Frequency of cancer generally increases with age • Cancers are constantly arising in our bodies, but our immune system kills them off • With increasing age: -- Less effective immune system -- Less controlled cell division (more mutations) -- More exposure to carcinogens • Young age = sarcomas; old age = carcinomas • The major cancer deaths in children under 15 years of age: -- Leukemia -- CNS tumors -- Lymphomas -- Soft tissue sarcomas -- Bone sarcomas
Cancer Risk Increases with AgeLong-term exposure & less effective immune system Photo: Stevens A, Lowe J. Slide atlas of pathology. Mosby, London, 1995.
Trends in Cancer Incidence1930 - 2000 Photo: Kumar, Cotran, Robbins. Robbins Basic pathology, 7th ed., Saunders, Philadelphia, 2003.
Oral CancerAge- & Gender-Specific Incidence Rates Photo: Neville, et al. Oral and maxillofacial pathology, 2002.
CancerHereditary Factors • Hereditary predisposition toward cancer development is common • Inherited cancer syndromes -- 5-10% of cancers -- Often have specific molecular markers • Familial retinoblastoma: autosomal dominant (AD) -- 40% are familial -- 10,000x more risk • Familial adenomatous polyposis (FAP) of colon (AD) -- Gardner’s syndrome also has jaw osteomas • Colon cancer (other than FAP): familial
CancerHereditary Factors • Multiple endocrine neoplasia (MEN) syndrome (AD) • Neurofibromatosis types 1 and 2 (AD) • Breast cancer: familial; BRCA gene • Ovarian cancer: familial • Xeroderma pigmentosum: autosomal recessive (AR) • Ataxia telangiectasia: AR • Bloom syndrome: AR • Fanconi anemia: AR
Inherited Syndromes Associated with CancerAssociated Genetic Defect
Genetically Associated CancersThe cancer may not be in the mouth • Acanthosis nigricans • Ataxia-Telangiectasia • Cowden syndrome • Dyskeratosis congenita • Gardner’s syndrome • Gorlin syndrome (nevoid basal cell carcinoma syndrome) • Mucosal neuroma syndrome (MEN IIB, MEN III) • Neurofibromatosis • Peutz-Jeghers syndrome • Trisomy 21 (Downs syndrome) • Tuberous sclerosis • Xeroderma pigmentosum MEN (Multiple Endocrine Neoplasia) IIB or III.Painless yellow-white nodules of the tongue. Photo: ESTOP. .
Progression of CancerPathogenesis Photo: Kumar, Cotran, Robbins. Robbins Basic pathology, 7th ed., Saunders, Philadelphia, 2003.
Cancer PhenotypesGenetic Requirements • Self-sufficiency (promotes cell growth without signals) -- Mutated protooncogenes >> oncogenes >> oncoproteins (not regulated) • Cancer cells produce the same growth factors which influence them • Cancer cells create excess receptors to these growth factors -- e.g. excess epidermal growth factor receptors are in 80% of squamous cell carcinomas of lungs • Example: Overexpression of MYC protooncogene -- MYC is in nucleus of all cells -- When overexpressed: increased cyclin-dependent kinases (CDKs) to move cell cycle into an active phase (especially G1 to S) • Example: Mutation of RAS gene --Most common oncogene abnormality in tumors (30%) -- Cell is told to continue to proliferate Photo: Kumar, Cotran, Robbins. Robbins Basic pathology, 7th ed., Saunders, Philadelphia, 2003.
Cancer PhenotypesGenetic Requirements • Insensitivity to growth-inhibitory signals – TP53 (p53) tumor suppressor gene: exerts antiproliferation effects, regulates DNA-damage repair, regulates apoptosis; affected by stress -- TP53 is one of the most common mutations in cancers • Evasion of apoptosis • Limitless replicative potential – Telomere length maintenance is seen in virtually all cancers
Cancer PhenotypesGenetic Requirements Oncogenes in Neoplastic Transformation Increased Expression of Growth Factor Receptors Photos: Stevens A, Lowe J. Slide atlas of pathology. Mosby, London, 1995.
Cancer PhenotypesGenetic Requirements Mutation in Transducer Protein Gene Mutant Transcription Factor Production Photos: Stevens A, Lowe J. Slide atlas of pathology. Mosby, London, 1995.
Cancer PhenotypesGenetic Requirements Over-Production of Factors that Prevent Cell Death Photo: Stevens A, Lowe J. Slide atlas of pathology. Mosby, London, 1995.
Cancer PhenotypesGenetic Requirements • Development of sustained angiogenesis – Cannot metastasize without angiogenesis – When the angiogenic switch is turned on: cancer proliferations and then metastasis • Ability to invade and metastasize -- Tumor cells must detach from themselves, attach to stroma >> degrade/destroy the stroma (via metalloproteinases) >> migrate • Some tumors show organ tropism (metastases favor certain organs) -- Related to adhesion moleculesand receptors
Karyotype Changes in Cancer • Balanced translocations -- Philadelphia chromosome (chronic myelogenous leukemia) -- Usually 22 & 9 -- Burkitt lymphoma (usually 8 & 14) -- Follicular B-cell lymphoma (usually 14 & 18) • Deletions (more common in solid tumors) -- Retinoblastoma (13q) -- Colorectal carcinoma (17p, 5q, 18q) • 3. Gene amplification -- neuroblastoma -- Breast cancer (N-MYC and HER-2 genes)
Carcinogenesis • Major problem: nonlethal genetic damage or mutations • Probably “cause” 65% of all cancers -- Heredity is “cause” of 26-40% • Carcinogens: -- Chemical -- Radiant energy -- Microbial agents • Carcinogenesis is a multistep phenomenon (tumor progression) – Involves genes regulating DNA repair, angiogenesis, invasion, metastasis
Carcinogenesis • Three classes of regulatory genes are the main targets: 1) Protooncogenes (promote growth) -- Mutant alleles = oncogenes (dominant genes) 2) Antioncogenes (growth-inhibiting cancer suppressor genes) -- Tumor suppressor genes -- Both alleles must be damaged (recessive oncogenes) 3) Genes controlling apoptosis (programmed cell death) • DNA repair genes affect cell proliferation and survival -- If disabled: widespread mutations Photo: Kumar, Cotran, Robbins. Robbins Basic pathology, 7th ed., Saunders, Philadelphia, 2003.
CarcinogenesisIonizing Radiation Photo: Kumar, Cotran, Robbins. Robbins Basic pathology, 7th ed., Saunders, Philadelphia, 2003.
Human Papillomaviruses in Oral Lesions24 genotypes have been isolated from oral lesions & mucosa Herpes simplex virus was a red herring? * genotypes in bold yellow are isolated in at least 1/3 of all cases with HPV