Download
1 / 39
390 likes | 694 Views
The Vaccines for the Future. 2007. Kuan Mei-Mei. Centers for Disease Control, DOH, Taiwan. Oct 25, 2007. Outline. We already have the flu vaccines, why do we need another ones for the future? Development, Progress, evaluation and Entering clinical trials of the New flu vaccines

E N D
The Vaccines for the Future 2007 Kuan Mei-Mei Centers for Disease Control, DOH, Taiwan Oct 25, 2007
Outline • We already have the flu vaccines, why do we need another ones for the future? • Development, Progress, evaluation and Entering clinical trials of the New flu vaccines • Trend of Vaccine to fight against influenza pandemic • Future challenge: What we do not yet have (against HIV, Dengue…)?
Why new flu vaccines? • The seasonal flu is threat all of us especially causing great burden to elderly and children, annually. • Immunity duration of the current seasonal flu vaccine is about 1 year, duo to the virus’s antigenic drift. • Occurring of next pandemicis inevitable causing by virus’s antigenic shift.
Progress in new vaccines 1. Vaccine type: design and prepare a novel seed vaccine • Whole organism (killed virus; attenuated live virus by reverse genetics or by chemical processing) • Subunit vaccine i.e. component vaccine or Split virus:(DNA vaccine: a segment DNA cloning into a recombinant vector; recombinant proteins vaccines: which can mass produce in mammalian cell, insect cell, yeast or E. coli via proper vector)
2. Vaccine formula: ~ monovalent-, bivalent- or trivalent- antigens ~ adjuvant (immunity stimulant) adding: for antigen-sparing or immunogenicity-increasing ~ preserve-adding in multiple-doses package to inhibit microorganism’s contamination or preserve-free in single-dose 3. Deliver route ~ needle: i. m. ~ needle free: orally or nasal spray
Evaluation of new vaccines • Regulatory/Good Manufacturing Practice (GMP)/ Licensing issues in vaccine development • Animal models (preclinical stage) to test vaccine efficacy • Entering early clinical trial ~Safety: ~Immunogenicity: cellular immunity humoral immunity
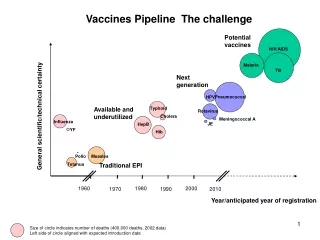
Ongoing Development of the Candidate Influenza vaccine for the future~ the trend of Vaccine to fight against influenza pandemic
Clinical trials • Phase I (n=20-80) - The randomised, double-blind, placebo-controlled, multi-centre(in one more places) trial - safety: adverse reaction record - immunogenicity : humoral and cellular immunity • Phase II (n=100-300) - age impact - increased power for safety and efficacy • Phase III (n=1,000-3,000) - final vaccine efficacy: incidence of flu at long term • Licensing • Phase IV - post marketing studies
Effectiveness of Influenza Vaccine in the Community-Dwelling Elderly • During 10 seasons, 713,872 person-seasons of observation • Influenza vaccination wasstatistically significant associated withboth reductions in the risks of hospitalization (a 27% reduction:odds ratio, 0.73; 95% confidenceinterval [CI], 0.68 to 0.77)and death (a 48% reduction: odds ratio, 0.52; 95% CI, 0.50 to 0.55) in the community-dwelling elderly. • Methods Logisticregression was used to estimate the effectiveness of the vaccine”for “the prevention of hospitalization for pneumonia or influenzaand death” after adjustment for important covariates. (Data were pooled from 18 cohorts of community-dwellingelderly members of one U.S. health maintenance organization(HMO) for 1990–1991 through 1999–2000 and of twoother HMOs for 1996–1997 through 1999–2000.). (Kristin L. Nichol et. al. 2007. V.357(14):1373-1381 )
Estimation of potential global pandemic influenza mortality • Methods identified all countries with high-quality vital registration data for the 1918–20 pandemic and used these data to calculate excess mortality. Developed ordinary least squares regression models that related excess mortality to per-head income and absolute latitude and used these models to estimate mortality had there been an influenza pandemic in 2004. • Findings Excess mortality data show that, even in 1918–20, population mortality varied over 30-fold across countries. • Per-head income explained a large fraction of this variation in mortality. Extrapolation of 1918–20 mortality rates to the worldwide population of 2004 indicates that an estimated 62 million people, 10th–90th percentile range (51 million–81 million) would be killed by a similar influenza pandemic; 96% (95% CI 95–98) of these deaths would occur in the developing world. If this mortality were concentrated in a single year, it would increase global mortality by 114%. • Interpretation This analysis of the empirical record of the 1918–20 pandemic provides a plausible upper bound on pandemic mortality. Most deaths will occur in poor countries—ie, in societies whose scarce health resources are already stretched by existing health priorities. (Christopher J L Murray et al. Lancer 2006)
Change perspective on immunization against influenza • Current influenza vaccine making strategies against influenza rely on decades old technology of virus strain selection and prolonged labor-intensive, embryonated chicken–egg based production methods. • Focusing on major surface glycoproteins, hemagglutinin (HA) and neuraminidase (NA), the immunity engendered by these vaccines is dominated by the anti-HA response. • Immunity is short duration about one year: susceptible to failure resulting from significant antigenic drift or antigenic shift in the time elapsing from the selection of the vaccine candidate strain and wild-type virus exposure. • To broaden the immune response against influenza by inclusion both HA and slowly evolving NA or MA in a vaccine will reduce the vulnerability to antigenic changes in a potential emerging influenza virus. • Take alternative production technologies(e.g. reverse genetic, insect cells, and yeast system)to decrease vaccine producing times, cost and efficacy is needed. (Bert E. Johansson, 2007; Kuan, 2007)
Rational ` • A universal flu vaccine focus using "conserved“ proteins, • such as M2 or NP, an inner protein as major component HA(H1~H16) NA(N1~N9) M2(ion-channel) 8 viral RNA • Influenza viruses belonging to the Orthomyxoviridae family, are enveloped viruses with 8 segmented negative sense RNA genome surrounded by a helical symmetry shell. M2e(or protruding part of M2): It's an appealing target because the 23 amino acids that make up the ectodomain, M1(Matrix protein)
Matrix Protein 2 Vaccination and Protection against Influenza Viruses, Including Subtype H5N1 • prevent deaths from flu, • may not keep people from getting sick, the way conventional vaccines normally do (notes Couch). • M2 antibodies seem to work by binding to infected cells and promoting their clearance, instead of blocking the virus (which sports few M2 surface proteins) from infecting new cells, as traditional vaccines are thought to do. • mice, still get sick and lose some weight, although they do survive ? • A regular flu vaccine matches the circulating strain only 80% to 90% of the time and often doesn't work at all in the elderly, whose immune systems aren't good at making new antibodies--M2 vaccines are a possible replacement. • M2 vaccines may do as a backup to regular vaccines, perhaps as an added component in annual flu shots. (EID, Vol. 13, No. 3 • March 2007)
Acambis entering phase I trials of universal flu vaccine • MA-based subunit vaccines:Acambis in Cambridge, Massachusetts, designed the vaccine by attaching three copies of M2e to the HepB core,: an ingredient that also increases the body's immune response. (vaccine, Jan. 2007) • Acambis Plc (the British biotech company) first announced the product, known as ACAM-FLU-A, has the potential to be both a universal pandemic flu vaccine and part of a universal seasonal vaccine against all `A' strains . • The 80-patient(aged between 18 and 40 years)Phase I trial(A randomised, double-blind, placebo-controlled, multi-centre trial in the US)will be conducted in the U.S. and will investigate ACAM-FLU-A's safety, tolerability and ability to generate an immune response. Results are due around the end of this year.
Why Using the Reverse Genetic Approach? • Prepare a seed virus for vaccine production • Traditional strategies of vaccine production were not viable, the virulent virus killed embryonated chicken eggs and cell line. • Entirely recovery of recombinant influenza viruses • ~Construct a attenuated r-virus:Replace the“high • pathogenic component” in HA by DNA substitution • ~Construct a cold adapted r-virus polybasic amino acids : 8 residues
A Reverse Genetics Approach for Recovery of Recombinant Influenza Viruses Entirelyfrom cDNA • The 8-plasmid pol I-pol II system for the generation of influenza A virus. ( Eight expression plasmids containing the 8 viral cDNAs inserted between the human pol I promoter and the pol II promoter are transfected into eukaryotic cells) • Because each plasmid contains 2 different promoters, both cellular pol I and pol II will transcribe the plasmid template, which will result in the synthesis of viral mRNAs and vRNAs. • After synthesis of the viral polymerase complex proteins (PB1, PB2, PA, nucleoproteins), the viral replication cycle is initiated. • Ultimately, the assembly of all viral molecules directly (pol II transcription)or indirectly(pol I transcription and viral replication) derived from the cellular transcription and translation machinery results in the interaction of all synthesized molecules (vRNPs PB1, PB2, PA, nucleoproteins and the structural proteins HA, NA, M1, M2, NS2/NEP) to generate infectious influenza A virus. (Virol. 76(22): 11744–11747. 2002. Jackson et al)
Generation of influenza vaccine viruses on Vero cells by reverse genetics: an H5N1 candidate vaccine strain produced under a quality system
Responsiveness to a pandemic alert: use of reverse genetics for rapid development of influenza vaccines • Methods: Removing the polybasic aminoacids that are associated with high virulence from the haemagglutinin cleavage site of A/Hong Kong/213/03 using influenza reverse genetics techniques. • Findings:A reference vaccine virus was produced in Good Manufacturing Practice (GMP)-grade facilities in less than 4 weeks from the time of virus isolation. This virus proved to be non-pathogenic in chickens and ferrets and was shown to be stable after multiple passages in embryonated chicken eggs. • Interpretation: The ability to produce a candidate reference virus in such a short period of time sets a new standard for rapid response to emerging infectious disease threats. (RJ Webby et al. Lancet. April 2004)
The expression the hemagglutinin protein of H5N2 avian influenza virus in yeast • Full-length HA-encoding gene of H5N2 AIV inserted into a secretory pPICZalphaA vector and integrated into the genome of Pichia pastoris by heterologous recombination. • The HA protein (69kDa protein) secretion into the medium was induced with methanol, and was recognized by an anti-AIV-HA monoclonal antibody in Western blot assay. • This is the first report on the cleavage of HA(0) into HA(1) and HA(2) in the methylotrophic yeast P. pastoris. This possibly was due to digestion by proteases from P. pastoris based on the amino acid sequences at the predicted cleavage site, (326)R-X-K-R(329). With similar modifications to the eukaryotes, large quantity, proper antigenicity, and low cost, this expression system may provide a simple tool to produce HA proteins for further use in preparation of ELISA kits and subunit vaccines. (Wang CY, et al. J Virol Methods. 2007 Aug 27 )
Antigen targeting and adjuvancy schemes dendritic cells immune cells • Antigen targeting and adjuvancy schemes that respectively facilitate • delivery of antigen to dendritic cells and elicit their activation • (maturation) have been explored in vaccine development via a 25-nm • nano- particle vaccine.
Exploiting lymphatic transport and complement activation in nanoparticle vaccines (Pre-clinical) • After intradermal injection, interstitial flow transported ultra-small nanoparticles (25-nm) highly efficiently into lymphatic capillaries and their draining lymph nodes, targeting half of the lymph node–residing dendritic cells, via interstitial flow and activating these cells by in situ complement activation, whereas 100-nm nanoparticles were only 10% as efficient. • The surface chemistry of these nanoparticles activated the complement cascade, generating a danger signal in situ and potently activating dendritic cells. Using nanoparticles conjugated to the model antigen ovalbumin, demonstrate generation of humoral and cellular immunity in mice in a size- and complement-dependent manner. (Sai T Reddy et, Nature Biotechnology Published online: 16 September 2007)
Technologies for presentation of protein or peptide antigens as vaccines must address two fundamental issues • Efficient delivery of antigen to dendritic cells(surface receptors such as DEC205 or 33D1): through using monoclonal antibodies either fused with protein to the surface of microparticles(antigen-encoding DNA, virus-like particles or polystyrene nanobeads ), subsequent dendritic cell activation to trigger adaptive immunity. • Target peripheral dendritic cells in skin: To initiate adaptive immunity, adjuvants must induce dendritic cell maturation. It often by 'danger signals' that work through pathways of innate immunity such as activation of Toll-like receptors (TLRs) and inflammatory cytokine receptors. • Antigen delivery to lymph nodes(dendritic cells are present in much higher concentration ): provide an attractive alternative • Exploiting a biophysical mechanism—interstitial flow—to access the lymphatic system as a low-resistance delivery route that leads to lymph nodes. The lymphatic system constantly drains fluid and macromolecules from the interstitial space, creating smallinterstitial flows on the order of 0.1–1 m/s. Take advantage of this basic physiological phenomenon by using nanoparticlesare convected by this interstitial flow through the interstitial matrix into the draining lymphatic capillary bed.
Vical Receives Grant From NIH to Advance RapidResponsem (TM) DNA Vaccine Platform • The company has been awarded a three-year, $6.0 million grant from the NIAID, part of the National Institutes of Health (NIH), for further development of a DNA vaccine manufacturing process with the potential to produce several million doses of vaccines in a matter of days. • It is ideally suited to enable an immediate response against emerging diseases affecting large populations, such as a pandemic influenza or SARS." About the RapidResponse(TM) Platform • The standard manufacturing methods that are being used to produce conventional vaccines take several months to several years and require specialized, capital-intensive facilities,", The RapidResponse (TM) system is designed to allow extremely rapid and large-scale production of DNA vaccines with low capital requirements. • The RapidResponse (TM) DNA vaccine manufacturing platform is intended to significantly reduce the time required to develop, manufacture and deploy vaccines against emerging diseases during the early stages of an infectious outbreak. By using a cell-free manufacturing process, the company believes that the RapidResponse(TM) DNA platform can overcome the time, capacity and cost challenges of manufacturing conventional vaccines for diseases such as influenza, which use killed or disabled viruses grown in chicken eggs or via cell culture, requiring months of production time in large, dedicated facilities. • (Vical Incorporated June 12, 2007 announced)
Adjuvantation is an important antigen-sparing strategy Adjuvant for antigen-sparing: oil-in-water–based emulsion; the oil phase is DL-alpha-tocopherol or vitamin E in Squalene, the water phase is polysorbate 80 (a nonionic detergent)。
Methods Two doses of an inactivated split A/Vietnam/1194/2004 NIBRG-14 (recombinant H5N1 engineered by reverse genetics) vaccine were administered 21 days apart to eight groups of 50 volunteers aged 18–60 years.. Blood samples were collected to analyse humoral immune response. Safety analyses were of the whole vaccinated cohort and immunogenicity analyses per protocol. The safety and immunogenicity of a recombinant H5N1 split-virion vaccine formulated with a proprietary adjuvant system and whether it can induce cross-reactive immunity is assessed. Findings All eight vaccine formulations had a good safety profile. The adjuvanted formulations were significantly more immunogenic than the non-adjuvanted formulations at all antigen doses. At the lowest antigenic dose (3·8 μg), immune responses for the adjuvanted vaccine against the recombinant homologous vaccine strain (A/Vietnam/1194/2004 NIBRG-14, clade 1) met or exceeded all US Food and Drug Administration and European Union licensure criteria. 37 of 48 (77%) participants receiving 3·8 μg of the adjuvanted vaccine seroconverted for neutralising antibodies against a strain derived genetics from a drifted H5N1 isolate (A/Indonesia/5/2005, clade 2). Adjuvantation conferred significant antigen sparing that could increase the production capacity of pandemic influenza vaccine. Moreover, the cross-clade neutralising antibody responses recorded imply that such a vaccine could be deployed for immunisation before a pandemic. (Isabel Leroux-Roels et al . Lancet 2007; 370: 580–89) Antigen sparing andcross-reactive immunity with an adjuvantedrH5N1 prototype pandemic influenza vaccine: Four antigen doses (3·8 μg, 7·5 μg, 15 μg, and 30 μghaemagglutinin) given with or without adjuvant
Further prospective Many other novel vaccines are ongoing to fight against more EID (e.g. HIV, Malaria, TB, Dengue, …)
HIV vaccine failure prompts Merck to halt trial ! • An HIV vaccine, Merck's STEP vaccine, being developed by Merck has apparently failed, causing the company to halt a large and once-promising clinical trial last week. • Using a mixture of components from three weakened adenoviruses to carry three synthetically produced HIV genes. The hope was that each gene would stimulate an immune response against the virus, as earlier trials had suggested. • The latest trial began in 2004 and enrolled 3,000 people considered to be at high risk of infection. But a group of 741 volunteers who received the vaccine saw 24 HIV infections, compared with the control group of 762 people who saw 21 infections. Furthermore, the vaccine did not reduce the amount of HIV in the bloodstream of those infected. Nature 449, 390 (27 September 2007)
Malaria research should go 'back to basics'Too many ineffectual vaccines threaten vital work • A report released on 17 September by the George Institute for International Health in Sydney, Australia. • Looked at the status and future prospects of 47 vaccines and 21 drugs in various stages of development. The vaccine furthest along is one developed by GlaxoS mith Kline (GSK). It should enter large-scale, phase III trials in 2008, with licensing pegged for 2012. The vaccine nearly halved severe malaria in a 2005 trial in 2,000 children younger than 5 years in Mozambique (P. L. Alonso et al. Lancet 366, 2012-2018; 2005). But the report comes down hard on the other vaccines. Far too many have been tested in clinical trials, in which most are certain to fail, eating up resources, says lead author Mary Moran, director of health policy at the George Institute.
Vaccine assembly from surface proteins of Staphylococcus aureus • Staphylococcus aureus, a Gram-positive bacteria is the most common cause of 60% of community and 80% hospital-acquired infection. It is commensal of human skin and nares, is the leading cause of bloodstream, lower respiratory tract, and skin/soft-tissue infections. The broad spectrum of important staphylococcal diseases also includes endocarditis, septic arthritis, toxic-shock syndrome, scalded-skin syndrome, and food poisoning. Because of the emergence of antibiotic-resistant strains, these infections represent a serious public health threat. • To develop a broadly protective , the cell wall-anchored surface proteins of S. aureus as antigens in a murine model of abscess formation is tested. • Immunization with four antigens (IsdA, IsdB, SdrD, and SdrE) generated significant protective immunity that correlated with the induction of opsonophagocytic antibodies. When assembled into a combined, the four surface proteins afforded high levels of protection against invasive disease or lethal challenge with human clinical S. aureus isolates. • Purified capsular polysaccharide, types 5 and 8 (which represent 80% of all capsular types found in clinical isolates; showed promise when used as a conjugate in experimental animals or in patients with end-stage renal disease • Subunit s composed of individual surface proteins, for example, clumping factor A (ClfA), clumping factor B (ClfB), iron-regulated surface determinant B (IsdB), or fibronectin-binding protein (FnBP), generate immune responses that afford partial protection against S. aureus challenge of experimental animals.
BALB/c Mice (n = 10) were immunized with the combined (IsdA, IsdB, SdrD, and SdrE) or with PBS, then, challenged by intraperitoneal injection with clinical S. aureus isolates (3–10 x 109 cfu), and monitored for 7 days for survival. Immunization with the combined generates protective immunity against lethal challenge with five different clinical S. aureus isolates. • Four days after infection, animals were killed, and the kidneys were under observation. Negative control: revealed abscess formation immunized with the combined vaccine
TB Epidemiology The most recent estimates of the worldwide epidemic of tuberculosis are for 2004, when there were 8-9 million new cases and 1-7 million deaths. The worldwide annual incidence continues to increase in Africa because of the HIV epidemic, whereas it is stable or falling in all other regions shows the worldwide estimated incidence of tuberculosis. Source: WHO
Novel vaccines against tuberculosis • The effectiveness of the current Bacille Calmette Gurin (BCG) vaccine is partial, and that of treatment of latent tuberculosis is unclear in high-incidence settings. The routine diagnostic methods that are used in many parts of the world are still very similar to those used 100 years ago. Multidrug treatment, within the context of structured, directly observed therapy, is a cost-effective control strategy. BCG confers some protection against tuberculosis in animal models. • During the past 10 years, vaccinologists have developed various novel vaccines with equal or greater efficacy than BCG in animals. Some of these candidates are now in phase I or II clinical trials, and the STOP-TB partnership intends to bring one such candidate into clinical use by 2015. Because childhood BCG vaccination has some effectiveness, a pragmatic consensus has emerged that novel vaccines should be assessed by how much more immunity they confer than does BCG.
Dengue infects at least 50 million people a year in more than 100 countries, mainly across Asia, Africa and South America. But unlike many diseases ravaging the developing world, dengue cuts across class.
Research frontline of dengue vaccine • GlaxoSmithKline (GSK), which is teaming up with the Walter Reed Army Institute of Research in Washington DC, and Sanofi-Aventis have both launched expanded clinical trials of vaccines in Asia and Latin America, with results expected by 2009. Trials with tens of thousands of participants would follow. • GSK's vaccine is a mixture of four live viruses that have been weakened in a process called attenuation. The viruses should provoke a lasting immune response, but not cause disease (R. Edelman et al. Am. J. Trop. Med. Hyg.69, 48–60; 2003). • Sanofi-Aventis has taken a different approach, genetically engineering a chimeric virus that contains molecular bits from each strain of dengue. (F. Guirakhoo et al. Vaccine19, 3179–3188; 2006). Nature 448, 734-735(16 August 2007)
A Build, own, operate (BOO) project for the production of flu vaccines in Taiwan • "Plan A" Taiwan has decided to ask that a deadline be set for the signing of a contract on a build, own, operate (BOO) project for the production of flu vaccines in Taiwan with Dutch Pharmaceutical company Akzo Nobel • The options for a "Plan B" have not yet be set, but could include signing contracts with another foreign vaccine maker to initiate a new BOO project; helping Taiwan's local companies to develop flu vaccines; and striking advance procurement agreements (APA) with foreign pharmaceutical companies to secure sufficient quantities of flu vaccines • D5K6805.CEP 10/14/07 16:31:23ENDITEM/jnc
Taiwan CDC : “Promoting humane vaccines R&D progress project (2006~2100)” • The goal is to construct the proper vaccine seeds including scale up four kinds of vaccines • Against four pathogens: (1) Influenza vaccine: and Academic sinica : a.inactivated whole virus (virus culture in MDCK cellsinactivation) cooperated with NHRI b. subunit vaccine : DNA vaccine (encoding Matrix protein), cooperated with Academic sinica (2) Enterovirus 71: virus culture in Vero cells inactivated whole virus (the culture volume scale up to 20L has been Technology shift to NHRI) (3)Japanese encephalitis virus: virus culture in Vero cells inactivated whole virus (virus’s purification Patent has been Technology shift to NHRI) (4)Neisseria meningitides group B: Among group A, B, C, W135 and Y, group B is the most dominant (80% in Taiwan epidemic) 1