Download
1 / 15
150 likes | 286 Views
NATIONAL TREATMENT AGENCY. Addiction to Medicines: Understanding Public Health Commissioning Beverley Oliver & Corinne Harvey Regional Managers , NTA North East and Yorkshire and Humber and the East Middlands. Slide 1. Workshop Programme 45mins :.

E N D
NATIONAL TREATMENT AGENCY Addiction to Medicines: Understanding Public Health Commissioning Beverley Oliver & Corinne Harvey Regional Managers , NTA North East and Yorkshire and Humber and the East Middlands Slide 1
Workshop Programme 45mins: • 5mins: Introductions from facilitators and from work shop participants. • 10mins: A short presentation to describe the landscape including realistic opportunities and threats - Setting the scene . • 30 mins: Small working groups to discuss and raise the poignant points for discussion - each group to feed back. • 5mins: Any further questions and close Slide 2
Contents: Understanding Public Health Commissioning • Public Health England and the Health and Care System • Commissioning Process • Opportunities and Support • Discussion and Questions Slide 3
Public Health England Slide 4
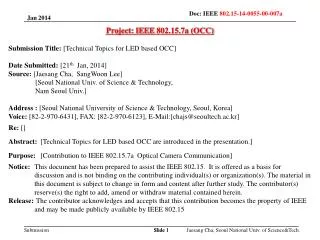
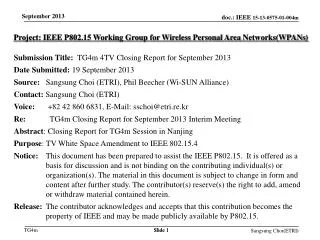
The new health and care system Local people and communities Police and Crime Commissioners could have a seat. Up to each LA Undertake JSNA & develop HWB Strategies setting out local priorities The evidence in this presentation can inform the JSNA and HWB Strategies. Health and Well-being Board Local Authorities CCG/NHS CB PHE Centres Responsible for publishing data and supporting delivery of PHOF Commissioning OF – set by the NHS CB for CCGs Accountability HealthWatch Oversight Links PHE NHS CB ASCOF Mandate – only means of holding the CB to account NHSOF PHOF Sets out the indicators that the PH system & DH understand are the best mechanisms to improve public health. Up to LAs to prioritise. Secretary of State for Health Parliament Sets out the indicators that the NHS should seek to achieve through the Mandate objective of continuous improvement Slide 5 5
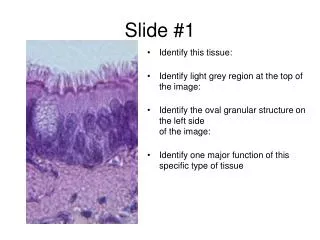
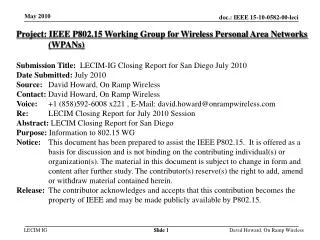
Commissioning Flowchart PHE needs assessment data Public Health Grant Engagement Opportunities Local needs assessment DsPH HWBBs JSNA & HWBS Operational Commissioners Local Performance Management Slide 6
Commissioning Process and the role of voluntary and statutory providers • ATM services commissioned by local authorities, through Directors of Public Health - supported by and coordinated through Health & Wellbeing Boards • Stronger together - describes how Health and Wellbeing Boards can work effectively with local providers is a framework for building health and wellbeing board and provider engagement • • A strategic, whole system approach – setting out a clear, strategic vision of how and why providers will be actively engaged in both determining and delivering the board’s priorities.. • • Clarifying the new commissioning landscape – and the benefits of the new partnerships to local providers and others. • • Involving providers in determining engagement approaches – this collaboration will foster better understanding, stronger cooperation and greater enthusiasm for more productive engagement. Slide 7
Opportunities and Support – Health and Wellbeing Boards • Provider-led initiatives – providers themselves have and can devise effective ways of how they can jointly engage with their health and • wellbeing board for mutual benefit. • Providers as board members – this can be applicable where health and wellbeing boards have been established as strategic bodies rather than direct commissioning structures. • A new kind of board and provider leadership is needed for all parties to work above their own organisation’s interests for the benefit of the local health and wellbeing system. • Different approaches and new skills may be required. • • Slide 8
Stronger together: how health and wellbeing boards can work effectively with local providers 04 • Informal peer to peer relationships are important and can be very effective engagement mechanisms outside of formal board meetings. • Market facilitation for innovation – boards will need to consult and engage with providers to stimulate service development and delivery design to better meet the needs of local populations. • Partnership links with local Healthwatch – building links between providers and Healthwatch will help to develop and create mechanisms and opportunities for engaging local communities and ensure their voices are heard on health and wellbeing boards. Effective engagement of local providers is significant to health and wellbeing boards fulfilling their role and responsibilities. If boards wish to transform, reconfigure and integrate their services to achieve improved health and wellbeing outcomes, it is essential they engage providers to make this happen. There are different mechanisms for making local provider engagement effective. Health and wellbeing boards should consider using and experimenting with a range of different approaches given the considerable variety of size and type of local providers. It will be important that no provider feels disadvantaged. Provider involvement in the design and development of engagement mechanisms will lead to stronger and more successful engagement across a board locality. Continued shared learning among health and wellbeing boards around the different engagement approaches being trialled and implemented locally will assist local areas to find the most appropriate methods to meet their engagement needs. Opportunities and Support – Health and Wellbeing Boards (continued) • Provider representation for groups, not single organisations – sitting on and engaging with health and wellbeing boards can reduce conflicts of interest, as representation is linked to a group not an individual provider, and be an effective way of feeding in provider knowledge and expertise. • Cooperative working with provider forums – health and wellbeing boards can engage with various provider forums but, to ensure proper engagement, partnership rather than consultation will be required to build collaborative working with providers. • Sub-groups of the health and wellbeing board – these groups, made up of commissioners and providers, can be effective at looking in more detail at a particular theme, care pathway or client group.
Opportunities and Support - Relationships • There is no statutory seat on the Health and Well-being Boards for voluntary and community sector representation, nor for specialist representation for the drug and alcohol sector. • However, HWBs are being encouraged to involve the VCS in the development of local strategies. The draft guidance on JSNAs and JHWSs published by the Department of Health for consultation in July 2012 explained that the local VCS could be represented on the HWB, and highlighted the potential for additional members, such as the VCS, service providers, health and care professionals, and representatives of criminal justice agencies ‘to bring expert knowledge to enhance JSNAs and JHWSs’. Slide 10
Opportunities and Support - Finance • Funding for drug and alcohol misuse treatment: • Drug and alcohol misuse prevention and treatment important part of public health responsibilities • 34% of national spend on public health has been on substance misuse - recognised in the target formula for the public health grants - illustrates significance of the agenda • Budget is the ring-fenced - but may be other local investment in services and local authorities will want to explore opportunities to lever in investment from elsewhere. • Activity and performance on drug treatment has had an impact on how much money an area has received • LAs required to report spending on an annual basis. There are categories for adult drugs, adult alcohol and YP drug and alcohol spending. Disinvestment will be very evident • Drug treatment continues to be a key priority for the government and this is unlikely to change Slide 11
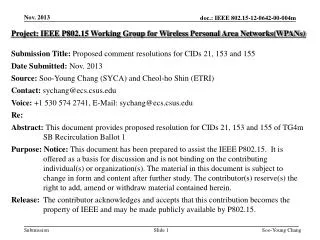
Where can PHE support? NTA’s/PHE JSNA documents Evidence base - growing To work with local PHE Drug and Alcohol teams in how to inform and influence planning (who, where, how?) Have your input via JSNA (contributing local data/intelligence) Support with case studies and local practice examples Scope and be aware of what contracts/funding may become available (ads/tenders primarily but could involve prime provider and subs, integrated services, etc.) Consider working with other providers to prepare joint tenders where appropriate Other solutions such as offering yourself as a sub-contractor Keeping in mind other relevant sources of funding: mental health (CCGs), voluntary sector (LA, charitable trusts, Lottery, companies, etc.) Identifying and presenting ‘Need’ to Commissioners
Any Questions? Thank you for your time and any questions? Slide 15