Download
1 / 28
290 likes | 534 Views
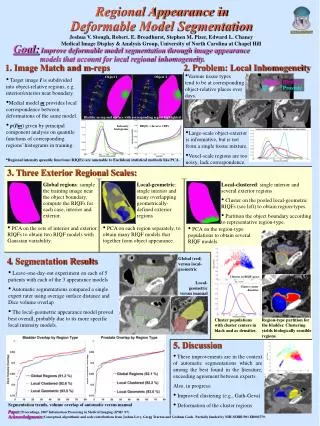
Segmentation of Tracheal Rings in Videobronchoscopy combining Geometry and Appearance. Carles S á nchez, Debora Gil , Antoni Rosell , Albert Andaluz and F.Javier Sánchez csanchez@cvc.uab.cat. OUTLINE. WHAT IS A BRONCHOSCOPY?. Bronchoscopy machine. Bronchoscopy procedure.

E N D
Segmentation of Tracheal Rings in Videobronchoscopy combiningGeometry and Appearance Carles Sánchez, Debora Gil, Antoni Rosell , Albert Andaluzand F.Javier Sánchez csanchez@cvc.uab.cat
WHAT IS A BRONCHOSCOPY? Bronchoscopy machine Bronchoscopy procedure Bronchoscope device • HDCC color camera that it is introduced inside the patient pathway. • It can be introduced through either nose or mouth.
WHAT IS A BRONCHOSCOPY? • Inside navigation system that provides realistic videos of the interior of the respiratory pathway. Trachea scheme Videobronchoscopy
WHAT IS A BRONCHOSCOPY FOR? Requirements 2D & 3D measurements from videos • Detect tumours • Estimate the percentage of obstructed airway (stenosis) • Determine the 3D size of tracheal stent Videobronchoscopy allows clinicians to:
HOW DO PHYSICIANS INFER MEASUREMENTS? • Tracheal rings are the main anatomical structures used to perform measurements of airway segments size and degree of stenosis. Reference Ring % obstruction Healthy segment Obstructed segment
CURRENT APPROACHES Contact procedure Video inspection - Images in perspective projection hinder 3D measures - Requires high experience and anatomical knowledge of the doctor • - Invasive procedure that requires intervention • Can cause lesions to soft tissues
EFFICACY OF CURRENT APPROACHES 30% Of wrongmeasurements that require repeating the whole intervention (re-measure & stent replacement) Requiresat least two new patient interventions Physicians need computer vision tools providing objective measurements [S. Norwood, et al., “Incidence of trachealstenosis and otherlatecomplicationsafterpercutaneoustracheostomy,” Annals of surgery, 232(2), 233, 2000] [J.M. Vergnon, et al., “Efficacy of tracheal and bronchial stent placement on respiratory functional tests,” Chest, 107(3),741–746, 1995]
GOAL • Automatic detection of tracheal rings using image processing tools • Challenges: 1) Variety of acquisition devices: resolution, flexible or rigid bronchoscope 2) Illumination & acquisition artifacts : surgical devices, illumination, blurred images and camera position 3) Image intensity appearance is not enough to discriminate rings to other structures: veins, carina...
OUR CONTRIBUTIONS Model of tracheal rings that combines their appearance and geometric features in videobronchoscopic images in order to minimize de impact of non-tracheal ring structures
TRACHEAL RINGS MODELLING • Tubular structure in conical projection • Analyzing Intensity profiles, rings can be described: • Appearance : • Ridge-Valley pattern • Geometry : • Concentric disposition • Increasing radial thickness Real trachea frame Radial intensity profile
APPEARANCE MODEL • Detection of valleys as trachealrings • Convolve the image with a bank of second derivatives of anisotropic Steerable Gaussian Filters (SGF) to account for orientation (Ɵ) and scale (σ) • Account for non-uniform illumination artifacts by the use of a normalized convolution (NSGF). σ [W.T. Freeman, et al. “The design and use of steerablefilters,” IEEE Transactions on Patternanalysis and machineintelligence, 13(9),891–906, 1991]
GEOMETRIC MODEL • Concentric disposition of rings around the carina • Change to polar coordinates Concentric disposition of rings around carina correspond to almost an horizontal orientation σmin (farthest ring) . . . σmax(closest ring)
GEOMETRICAL MODEL • Increasing radial thickness • It is detected by a decreasing scale profile as rings are traversed from most external part (L1 plot) • Structures not belonging to tracheal rings (carina, surgical devices..) break decreasing profile and are discarded. Image polar domain Maximum response of NSGF Higher intensity means larger scales
IMAGE PROCESSING SCHEME Input Preprocess StructureDescription FilteringStructure Preserving Diffusion Representation Space Ring Appearance Modelling Output Ring Geometric Modelling [Sánchez, C., Sánchez, J., Rosell, A., and Gil. Detecting tracheal rings in videobronchoscopy images. CVCRD2011, pages 132–135.] [Sánchez, C., Sánchez, J., Rosell, A., and Gil, D. An illumination model of the trachea appearance in videobronchoscopy images. ICIAR2012]
EXPERIMENTAL SETUP • GOAL : Detection of trachealrings • Dataset : 4 sequences
EXPERIMENTAL SETUP • GOAL : Detection of tracheal rings • Dataset : 4 sequences • Results by comparison with manual segmentation by medical expert • Two different experts in order to account inter-observer variability. • Accounting Sensitivity (Sens) and Precision (Prec) 1 pixel distance away from manual curves. • Mean ±standarddeviation for each sequence. • Wilcoxon signed-rang test to compute the differences between experts and automatic.
RESULTS – Quantitative • Wilcoxon test : confidence intervals of the difference (AUT-IO) • P-val~ 0 : indicates that differences are significant. • Else : Automatic segmentations are detecting as manual ones.
RESULTS – Qualitative • All rings are detected (sensitivity within inter-observer range) • Some extra structures dropping precision • Rigid artifacts • Some rings well detected but not identified by the expert (external and internal ones)
RESULTS – IO Variability • Some inner and outer rings not identified by experts. • Continues lines because of the doctor knowledge
RESULTS vs. Basic intensity aproches Basic intensity approaches Geometry and appearance model
CONCLUSIONS & FUTURE RESEARCH CONCLUSIONS: • Tracheal ring detection for stenosi assessment is a challenging task and novel area. • We have introduced a Geometrical Appearance model for tracheal ring detection. • Our geometric structure avoids any response at the carina and minimizes the impact of alien structures (veins, blood, surgical devices...). • Results prove that our detection can retrieve most clinically relevant tracheal rings • Enlarge the dataset including more types of pathologies, rigid and flexible • Suppress all responses in the rigid artifacts • Close the detected rings FUTURE RESEARCH:
Segmentation of Tracheal Rings in Videobronchoscopy combiningGeometry and Appearance THANKS FOR YOUR ATTENTION!! ? Carles Sánchez, Debora Gil, Antoni Rosell , Albert Andaluzand F.Javier Sánchez csanchez@cvc.uab.cat