Download
1 / 26
270 likes | 343 Views
Cytomegalovirus DR.K.RAJA GHTM CHENNAI. LEARNING OBJECTIVES. CMV IN IMMUNO COMPETENT PATIENTS CMV IN IMMUNO COMPROMISED PATIENTS CMV IN PREGNANT WOMEN. KEY POINTS. IN HIV CMV IS REACTIVATION OF LATENT INFECTION HIV AND CMV COINFECTION – RAPID PROGRESSION OF HIV

E N D
LEARNING OBJECTIVES CMV IN IMMUNO COMPETENT PATIENTS CMV IN IMMUNO COMPROMISED PATIENTS CMV IN PREGNANT WOMEN
KEY POINTS • IN HIV CMV IS REACTIVATION OF LATENT INFECTION • HIV AND CMV COINFECTION – RAPID PROGRESSION OF HIV • CD4 - <50 – CMV IS ACTIVATED AND DISSEMINATED • IN PREGNANCY ONLY PRIMARY INFECTION CAUSES IN VITRO TRANMISSION • NEONATES, INFECTED IN UTERO - RASHES, HEPATITIS, GASTROENTERITIS AND A ORGAN SPECIFIC MALADIES. • SURVIVORS – HEARING LOSS, VISION IMPAIRMENT AND MENTAL RETARDATION. • IN IMMUNO COMPETENT – FLU LIKE SYNDROME • AND REMAIN LATENT LIFE TIME
Human Cytomegalovirusherpesvirus betaherpesvirinae subfamily CMV infected cells may become enlarged (cytomegalia), showing intranuclear inclusions.
Virus StructureEnveloped, slightly pleomorphic Spherical 120 – 200 nm in diameter CapsidEnvelopeTegumentGenomedouble stranded DNA per virion
TRANSMISSIONTransmitted through infected bodily fluids that come in contact with hands and then are absorbed through the nose or mouth of a susceptible person.
Transmission can also occur – congenitally - by sexual contact - through blood transfusion
CMV may be shed in the bodily fluidsurine saliva bloodsemen breast milkThe shedding of virus- intermittent- without signs-without causing symptoms.
CMV infectionHigh-risk groups: (1) infection to the unborn baby during pregnancy(2) infection to people who work with children (3) immunocompromised person:a) organ transplant recipients b) human immunodeficiency virus (HIV)C)undergoing hemodialysisd) patients with cancer
The primary infection presents as mononucleosis-like syndrome which soon resolves. Most of them asymptomatic for life. CMV IN IMMUNO COMPETENT PERSONS
IN PREGNANCY WHEN A WOMEN WHO HAS NEVER HAD CMV INFECTION BECOMES INFECTED WITH CMV, THERE IS A POTENTIAL RISK THAT AFTER BIRTH THE INFANT MAY HAVE CMV-RELATED COMPLICATIONS IN PREGNANCY
NEONATES, INFECTED IN UTERO - RASHES, HEPATITIS, GASTROENTERITIS AND A ORGAN SPECIFIC MALADIES.THE MOST COMMON OF WHICH ARE ASSOCIATED WITH HEARING LOSS, VISUAL IMPAIRMENT, OR DIMINISHED MENTAL AND MOTOR CAPABILITIES. NEONATES
INFANTS AND CHILDREN WHO ACQUIRE CMV AFTER BIRTH HAVE FEW, IF ANY, SYMPTOMS OR COMPLICATIONS.
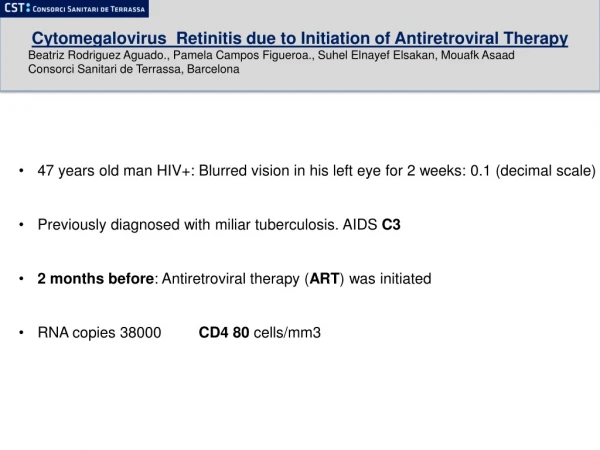
Primary infection - rare in HIV as most have been exposed to CMV Latent CMV infection is activatedin advanced HIV disease. CMV IN HIV INFECTION
CMV IN HIV retinitis oesophagitis encephalitis myelitis radiculopathy colitis pneumonitisadrenalitispancreatitis
CMV Retinitis small floaters foggy or blurred vision loss of central or peripheral vision routine exam when the infectious process is early and located in the peripheral retina loss of vision retinal detachment
CMV – COFACTOR IN THE PROGRESSION OF HUMAN IMMUNODEFICIENCY VIRUS TYPE 1 (HIV-1) DISEASE. PROGRESSION
Laboratory tests CMV antibody - paired serum samples1) ELISA2)fluorescence assays 3)indirect hemagglutination4)latex agglutination
A virus cultureTissue biopsy for cultureCMV blood culture ("buffy coat" culture)CMV urine culture CMV sputum cultures
ANTIGENCMV shell vial (a method of determining the presence of CMV antigens) BIOPSYBiopsies of organs likely to be infected with CMV
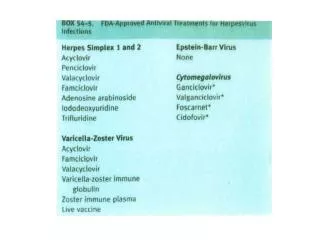
TreatmentFirst line:ganciclovir, powder for injection, 500 mg in vial Adults: 5 mg/kg i.v twice a day for 14-21 daysSecond line:foscarnet,solution for injection, 24 mg/ml 250 ml, 500 mlAdults: retinitis; 90 mg/kg i.v daily for 14-21 days for CMV Adults: CMV oesophagitis; 90 mg/kg i.v twice a day for 14-21 days
Maintenance First Line:ganciclovir,capsules, 250 mgAdults: 1 g orally three times a daySecond Line:ganciclovir, powder for injection, 500 mg in vialAdults: 5 mg/kg i.v dailyThird line:foscarnet,solution for injection, 24 mg/ml 250 ml, 500 mlAdults: 90 mg/kg i.v daily
ALTERNATIVE TREATMENTValganciclovir 900mg bid poCidofovir 5mg/kg weekly
PROPHYLAXIS Primary prophylaxis is generally not recommended because of cost concerns, inconvenience and the potential for development of resistanceMAINTAINENCECD4+ cell counts > 100 for > 3 months as a result of potent ART
Prevention Simple hand washing with soap and water is effective in removing the virus from the hands.