Download

1 / 79
800 likes | 817 Views
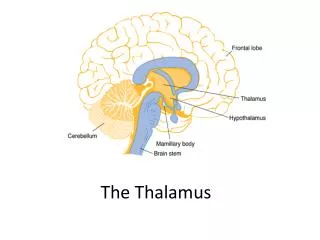
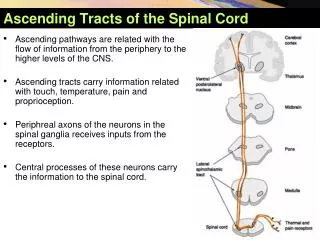
Brain Death Clinical evaluation & Ancillary tests P.Sariaslani. MD Assistant Professor of Neurology Medical College of Kermanshah. The state of consciousness (arousal). The ascending RAS , from the lower border of the pons to the ventromedial thalamus

E N D
Brain DeathClinical evaluation & Ancillary testsP.Sariaslani. MD Assistant Professor of Neurology Medical College of Kermanshah
The state of consciousness (arousal) • The ascending RAS, from the lower border of the pons to the ventromedial thalamus • The cells of origin of this system occupy a paramedian area in the brainstem
To cause coma, as defined as a state of unconsciousness in which the eyes are closed and sleep–wake cycles absent • Lesion of the cerebral hemispheresextensive and bilateral • Lesions of the brainstem: above the lower 1/3 of the pons and destroy both sides of the paramedian reticulum
Normal Brain Anatomy Cerebral Cortex Reticular Activating System Brain Stem
Brain Stem Midbrain Cranial Nerve III • pupillary function • eye movement
Brain Stem • Pons • Cranial Nerves IV, V, VI • conjugate eye movement • corneal reflex
Brain Stem • Medulla Cranial Nerves IX, X • Pharyngeal (Gag) Reflex • Tracheal (Cough) Reflex • Respiration
In most adult series, trauma and subarachnoid hemorrhage are the most common event leading to brain death. Others include intracerebral hemorrhage, hypoxic ischemic encephalopathy, and ischemic stroke. Any condition causing permanent widespread brain injury can lead to brain death.
Causes of Brain Death Normal Cerebral Hemorrhage
Causes of Brain Death Cerebral Anoxia Normal
Causes of Brain Death Subarachnoid Hemorrhage Normal
Causes of Brain Death Normal Trauma
Causes of Brain Death Meningitis Normal
Mechanism of Cerebral Death ICP>MAP is incompatible with life Increased Intracranial Pressure
Conditions Distinct From Brain Death • Persistent Vegetative State • Locked-in Syndrome • Minimally Responsive State
Vegetative state (coma vigil, apallic syndrome) • Patients who survive coma do not remain in this state for > 2–3 weeks, but develop a persistent unresponsive state in which sleep–wake cycles return. • After severe brain injury, the brainstem function returns with sleep–wake cycles, eye opening in response to verbal stimuli, and normal respiratory control.
Locked in syndrome • Patient is awake and alert, but unable to move or speak. • Pontine lesions affect lateral eye movement and motor control • Lesions often spare vertical eye movements and blinking.
Vegetative Locked-in
Minimally Responsive State Static Encephalopathy • Diffuse or Multi-Focal Brain Injury • Preserved Brain Stem Function • Variable Interaction with Environmental Stimuli
Brain Death Neurological Examination Clinical Prerequisites: • Known Irreversible Cause • Exclusion of Potentially Reversible Conditions • Drug Intoxication or Poisoning • Electrolyte or Acid-Base Imbalance • Endocrine Disturbances • Core Body temperature > 32° C
To ensure that the cessation of brain function is “irreversible,” physicians must: • determine the cause of coma • exclude mimicking medical conditions • - observe the patient for a period of time to exclude the possibility of recovery
●Clinical or neuroimaging evidence of an acute CNS catastrophe that is compatible with the clinical diagnosis of brain death, ie, the cause of brain death should be known. ●Core temperature >36ºC (97ºF). Hypothermia may also confound the diagnostic assessment of brain death and can also delay the increase in PaCO2 necessary to complete the apnea test. ● There is little evidence base for a choice of threshold temperature. Canadian forum recommendations published in 2006 use 34ºC as a standard . ●Normal systolic blood pressure >100 mm Hg. Vasopressors may be required.
Brain Death Current Consensus • Absent Cerebral Function • Absent Brainstem Function • Apnea
Coma No Response to Noxious Stimuli • Nail Bed Pressure • Sternal Rub • Supra-Orbital Ridge Pressure
Absence of Brain Stem Reflexes • Pupillary Reflex • Eye Movements • Facial Sensation and Motor Response • Pharyngeal (Gag) Reflex • Tracheal (Cough) Reflex
Pupillary Reflex Pupils dilated with no constriction to bright light
Eye Movements Occulo-Cephalic Response “Doll’s Eyes Maneuver”
Oculo-Vestibular Response “Cold Caloric Testing”
Facial Sensation and Motor Response • Corneal Reflex • Jaw Reflex • Grimace to Supraorbital or Temporo-Mandibular Pressure
Confounding Clinical Conditions • Facial Trauma • Pupillary Abnormalities • CNS Sedatives or Neuromuscular Blockers • Hepatic Failure • Pulmonary Disease
Observations Compatible with Brain Death • Sweating, Blushing • Deep Tendon Reflexes • Spontaneous Spinal Reflexes- Triple Flexion • Babinski Sign
Dramatic spontaneous movements when severe hypoxia is attained upon terminal disconnection from the ventilator for Several minutes: These include opisthotonos with chest expansion that simulates a breath, elevation of the arms and crossing them in front of the chest or neck ( Lazarus sign ), head-turning, shoulder-shrugging, and variants of these posturing-like movements. For this reason the advice that the family not be in attendance immediately after mechanical ventilation has been discontinued.
:Confirmatory Testing - Recommended when the proximate cause of coma is not known or - when confounding clinical conditions limit the clinical examination