Download
1 / 11
110 likes | 300 Views
The Connective Tissue Oncology Society. Surgical Treatment of GIST post Imatinib. Barry W. Feig, M.D. Robert S. Benjamin, M.D. The SARCOMA Center. Chemotherapy + Surgery CR Chemotherapy CR Partial Response Stable Disease. SOFT TISSUE SARCOMAS 1971-1977

E N D
The Connective Tissue Oncology Society Surgical Treatment of GIST post Imatinib Barry W. Feig, M.D. Robert S. Benjamin, M.D. The SARCOMA Center
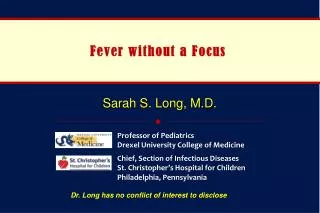
Chemotherapy + Surgery CR Chemotherapy CR Partial Response Stable Disease SOFT TISSUE SARCOMAS 1971-1977 Time to Progression - Distant Metastases 1.00 TOTAL FAIL 12 37 66 97 9 32 63 96 0.80 0.60 PROPORTION p = 0.64 p = 0.002 p = 0.002 vs vs 0.40 vs 0.20 0.00 0 1 2 3 4 5 6 7 8 9 10 YEARS
GIST: Management of Resistance • If the majority of tumor is controlled by imatinib mesylate, then continue therapy • Dose escalation up to 800-1000 mg/d as tolerated • Surgical resection of progressing sites if possible • Other trials Demetri et al. JNCCN. 2004;21(suppl 1):S1.
RADIOGRAPHIC RESPONSE TO IMATINIB IN RECURRENT / METASTATIC GIST (N=35)
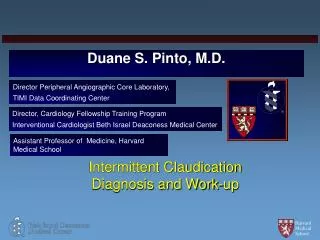
TIME OF SURGERY IN IMATINIB RESPONSIVE RECURRENT / METASTATIC GIST COMPLETE RESECTION (N=11) INCOMPLETE RESECTION (N=18) SURGERY SURGERY PROGRESSION Median (months) 10.0 18.0 23.7 P=0.04
GIST Surgery: Randomized Study • Surgery vs No Surgery • Surgery at maximum response vs Surgery at first evidence of relapse.
TIME OF SURGERY IN IMATINIB RESPONSIVE RECURRENT / METASTATIC GIST COMPLETE RESECTION (N=11) INCOMPLETE RESECTION (N=18) SURGERY SURGERY PROGRESSION Median (months) 10.0 18.0 23.7 P=0.04
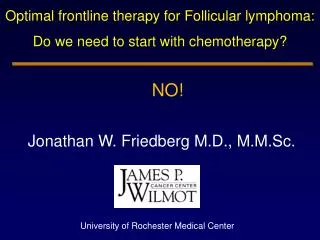
TIME OF SURGERY IN IMATINIB RESPONSIVE RECURRENT / METASTATIC GIST R A N D O M I Z E EARLY SURGERY PROGRESSION DELAYEDSURGERY Months (estimate) 10 18 20
GIST Surgery: Endpoints • Time to Progression from start of imatinib • If no difference, then surgery does not have a role • If TTP longer with early surgery, then surgery is adding • Survival • If no difference, delayed surgery is preferable (not all will need it). • If survival better with early surgery, it is better to do at that time.
The Connective Tissue Oncology Society Surgical Treatment of GIST post Imatinib Barry W. Feig, M.D. Robert S. Benjamin, M.D. The SARCOMA Center