Download
1 / 60
610 likes | 879 Views
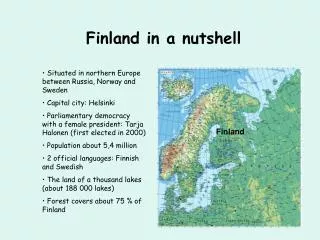
The AICD in a nutshell Reducing Shocks. By Nick Jackson. ICD TRIALS. ICD SHOCKS. CAUSES OF SHOCKS. reasons to reduce shocks. Quality of life improvement (≥5 shocks). Less pain, less shocks and less fear of getting shocks. Increased acceptance of ICD. May positively effect survival.

E N D
The AICD in a nutshellReducing Shocks • By Nick Jackson
reasons to reduce shocks • Quality of life improvement (≥5 shocks). • Less pain, less shocks and less fear of getting shocks. • Increased acceptance of ICD. • May positively effect survival. • Battery life improved. • Decreased cost to healthcare • Less ED visits, blood tests, calls to cardiologists, medications, ablations and hospitalisations.
Mortality of inappropriate shocks • SCD-HeFT and ALTITUDE analysis suggested inappropriate shocks increased mortality by up to 20% (may be damaging to the myocardium). • In a further analysis of ALTITUDE it was found inappropriate shocks for AF/flutter increased mortality (by 61%) but not so for ST or oversensing. • Mortality for appropriate shocks goes up more drastically. This is not so for VT/VF treated by ATP. • In ALTITUDE pts who failed ATP had more severe underlying CM, worse CCF, more rapid VT/VF and more PMVT which may have been the driving force for greater mortality. 1
shocks in altitude • 3809 of 28000 pts in ALTITUDE received shocks over 3.1 years. • AF/flutter (18%), ST/SVT (17%), noise/artifact/oversensing (5%), MVT (36%), PMVT (16%), MVT&PMVT (7%), NSVT (1%). • Hazard ratio for mortality, by rhythm at the time of shock, compared to mortality after a shock for AF/flutter: 1
SHOCKS in ALTITUDE • Second analysis of 3630 pts receiving shocks with matched patients who did not receive shocks. • The Increase in mortality for inappropriate shocks is confined to the AF/flutter group. • Need to look at the underlying rhythm and treat that, especially if it is AF/flutter with rapid ventricular rates. 1
methods for shock reduction • Unnecessary shocks • For VT episodes that would have terminated safely of their own accord or with ATP • Inappropriate shocks • Given for non VT/VF episodes
ATP • There is still some thought that the interaction of shocks and VT in a myopathic heart may lead to faster cardiac deterioration (troponins tend to be elevated after both). • There is no evidence that VT terminated with ATP is associated with increased mortality. • ATP reliably terminates VTs ≤200 bpm (CL 300ms) in 90% of pts. • Concern over ATPs efficacy for faster rates: Tendency to accelerate VTs, syncope during ATP, premature treatment of NSVTs or delaying shocks for life threatening VTs. 2
Pain free II • Pts were randomised to ATP or initial shocks for FVT (200-250 bpm). • ATP was successful 72% of the time in this group. 68% of the time for VT 214-250 bpm. • Rates of acceleration were low (2% vs 1%) and rates of arrhythmic syncope were also low (0.7% in both groups). • No clinical difference in episode duration or sudden death but improved quality of life c/w the shock group. 2
PAIN FREE II • This study used 18/24 intervals for VF/FVT and found that NSVT was not a predictor of ATP success. • Arrhythmic syncope did not increase with this detection interval c/w PAIN FREE I. Many factors explain the haemodynamic response to VT making it heterogeneous. • Shocks are associated with significant morbidity, contributing to anxiety syndromes in 15-38% of ICD pts. This trial was the first to show improved QoL with ATP, largely due to mental well being. 2
ATP • ATP has since become nominal in ICDs. • They now can deliver a single sequence of ATP during charging so there is no delay in shock delivery for VF. • “The ICD is an ATP device with back up shocks.”
prepare trial • Followed 700 pts with AICDs for primary prevention and compared them to a matched cohort from the EMPIRIC and MIRACLE ICD studies. • VT/VF was detected for rates >182 bpm that was maintained for at least 30/40 intervals. ATP was the first therapy for regular rhythms 182-250 bpm. • SVT discriminators were used for rhythms ≤200 bpm. • High output first shocks (30-35J) 3
results 3
prepare programming • PREPARE programming can safely reduce the number of tachyarrhythmias subjected to shock therapy. • Slower, briefer arrhythmias usually don’t cause syncope or death but can cause haemodynamic compromise. • But ATP +/- Shocks for ST or AF with RVR can itself lead to haemodynamically compromising rhythms, ischaemia, EMD and possibly syncope, AMI or death. • Overall safety in this study was excellent as assessed by arrhythmic syncope, untreated VT and mortality. • Mortality estimates based on ICD detected episodes give elevated results. The prepare protocol better estimates those that were actually saved from SCD by their ICD. 3
oversensing/artifact • Lead integrity alert • Lead malfunction ~ 4.6% at 10 years. • Lead noise discrimination alert • Compares near field to far field. • T wave oversensing algorithm • Frequency/pattern/slew • Dynamic sensing.
AICD PART TWO • By Nick Jackson
SVT Discriminationalgorithms Programmed differently by different companies. • Single Chamber • Onset • Stability • Morphology • Dual Chamber • AV logic • Both • SVT limit (In the VF zone/discrimination in the VF zone) • Confirmation (after ATP and during charging)
programming • Sensitivity and specificity are proportional to each other and should be individualised to the pt. • The shorter the CL the less proportion of SVT. • Singe chamber ICDs: Onset, stability, morphology. • Onset. VT occurring during ST, exercise induced VTs. • Stability. Pseudo-regularisation of AF with RVR. Or irregular VTs. • Combined Onset and stability has been associated with a sensitivity of 100% and specificity of 83%. 6
programming • Medtronic morphology algorhythm as a sole discriminator: Sens of 98.6% and spec 78.2%. • St. Jude morphology discriminator, Spec 71-95% and sens 77- 94.4%. And combined with stability and onset for 2/3 it achieved sens 96% and spec 90.9%. • Guidant morphology (VTC) had sens 99% and spec 91-97%. • Template alignment is key. Truncation and septal VTs. • Specificity is proportional to the duration of follow up and sample size. Can’t directly compare these figures. 6
dual chamber icds • The ventricular rate exceeds the atrial rate in >90% of VTs. • Biotronik algorithm. V >A =VT. A >V then it looks at A and V stability and ratio of signals. If A =V then the algorithm looks at onset and stability. Reported sensitivity and specificity of SMART detection is 100% and 89% respectively. • Guidant Rhythm ID. If V > A =VT, otherwise the morphology algorithm is appraised. Both criteria for stability and atrial rate above a certain threshold are needed to diagnose SVT. Sens and spec are 100% and 92-97%. • Medtronic PR logic. (optionally programmed in combination with stability, onset and morphology). Looks at AV and VA interval patterns to discriminate VT vs SVT (places each V and A event into a bin according to timing). Sens 100% and spec 66-72%. 6
DUal chamber ICDs • St Jude. V > A =VT. If V =A then the AV interval is looked at to determine dissociation (VT arising during ST). Then onset and morphology is applied. If A >V then morphology and stability are applied with or without AV association criterion. Variations can be programmed individually as well. Sens 98.7-100% and spec 73.5 to 90.9%. • The RIGHT trial will be a direct randomised comparison but the results are not published as yet (Medtronic vs Boston Sci). • A large retrospective analysis showed more heart failure hospitalisations in pts with a Dc-ICD implanted. • The more important question isn’t which device to use but is the device appropriately programmed. 6
Specificity comparison Grey: Specificity from clinical data. Black: Specificity resulting from simulation when weighing SVT according to clinical prevalence. (Phylax AV, Defender, Ventak AVIII, Gem DR, Photon DR). 10
single vs dual • Atrial leads are useful where pacing indications exist. • Dual chamber ICDs significantly reduce inappropriately treated episodes (per episode analysis) compared with single chamber ICDs (30.9% vs 39.5%)(7). Without significantly increasing the number of patients receiving inappropriate discharges (per pt) in prospective analysis. • This was found to be cost effective as well. • Per patient analysis dual and single chamber ICDs have similar specificity. Dual chamber discriminators are prone to atrial undersensing errors which may be underestimated in trials. (Also crosstalk and atrial blanking). 8,9
single vs dual • If complications of dual chamber device implantation are limited and RV pacing is reduced- Dc-ICDs reduce clinically significant adverse events defined as all cause mortality, invasive intervention, hospitalisation for cardiovascular causes, inappropriate shocks and sustained symptomatic atrial tachyarrhythmias. • Higher rates of complications are consistently reported in the literature for Dc-ICD implantations. • Individualised decision. An atrial lead can be added for difficult patients who continue to have misclassified SVT with a single chamber device (history of difficult to control SVT). 8,9
Dual vs Single Pt’s receiving inappropriate therapies, 21% vs 18% for dual and single respectively. Number of atrial tachyarrhythmias that were inappropriately treated. 36% RRR from these pooled studies. 9
dual vs single Mean number of inappropriate therapies per patient, a reduction of 1.1 in the mean of inappropriately treated episodes. 9
Medications • Although the ICD aborts VT/VF, these episodes are frequently unpleasant/symptomatic. • 23% of pts dread shocks and 5% prefer to do without the ICD and ‘take their chances.’ • Medications may limit shocks due to SVT as well. May make VT more amenable to ATP, may make VT more responsive to shocks, decrease ED visits/hospitalisation and prolong battery life. • ≥70% of pts receive adjuvant drug therapy even though there is no formal indication for it. • Drug-device interaction. 4
medications • In the AVID study (antiarrhythmic versus ICD trial) 18% of pts in the ICD arm were started on drug therapy (amiodarone 42%, sotalol 21% and mexiletine 20%) to reduce shocks. • These crossover pts had an increased time to first event by ~7 months and reduced 1 year arrhythmia event rate from 90% to 64%. • Several studies have evaluated the use of antiarrhythmic drugs for prevention of ICD shocks, primarily in the setting of secondary prevention. 4
sotalol • Prospective multicentre study of 302 pts with ICDs randomly assigned to sotalol or placebo. • Sotalol lead to a reduction in death/inappropriate shock (HR 0.36, p=0.007) irrespective of LVEF or B Blocker usage. • Mean fqncy of all cause shocks was 1.43+/- 3.53 with sotalol and 3.89+/-10.65 in control. • 27% of pts in the sotalol group had it stopped early due to adverse events (usually B Blocker S/E’s) there was one episode of TdP. 4
sotalol 4
Beta Blockers • In a study by Pacifico et al. b blockers had no effect on event free survival, however, a study by Seidl et al. of 70 pts with ICDs assigned to sotalol or metoprolol found a positive effect. • Survival probability for reaching an end point of symptomatic VT/VF or death was better in the metoprolol group (83% and 74%) at 1 and 2 years c/w the sotalol group (47% and 38%, p=0.004). • ICD interventions (ATP/shocks) were significantly lower in the metoprolol group. • A similar study by Kettering et al. involving 100 pts found metoprolol and sotalol to be equivalent at reducing ICD interventions. • Similar efficacy of B Blockers was found in an analysis of the MADIT II trial where the response was dose related. 4
azimilide • Novel class 3 drug that blocks the rapid and slow components of the delayed rectifier K current. • Efficacy in atrial and ventricular rhythms and with LV dysfunction. • In the SHIELD study (double blind), 75mg and 125mg doses were evaluated in 633 ICD recipients. • Over a median of 367 days, all cause shocks and symptomatic arrhythmia terminated by ATP were significantly reduced with 75mg and 125mg (HR 0.43 and 0.53). • All appropriate shocks were also reduced. Incidence of ICD interventions per pt year were reduced from 25.1 (placebo) to 17.1 to 9.6 (on 75mg and 125mg of azimilide). 4
azimilide • All cause shocks were also reduced and 86% of study pts were receiving concomitant B Blocker therapy. • Azimilide also appeared to reduce VT storm, to reduce hospitalisations and had a similar tolerance profile to placebo. • TdP occurred in 5 azimilide pts and 1 placebo pt. It is currently under review by the FDA for this indication. Text 4
amiodarone • OPTIC study compared amiodarone + B blocker, B blocker and sotalol to prevent ICD shocks. • Pts in the 2 active groups had a reduced risk of shocks by 56% c/w B Blocker alone. Amio + B blocker was more effective than B blocker alone (HR 0.27, P<0.001) or sotalol (HR 0.43, P=0.02) in preventing all cause shocks. • There was a trend towards sotalol being superior to metoprolol. • Mortality was not statistically significant amongst all groups. • Discontinuation rates were 18.2% amio, 23.5% sotalol and 5.3% B blocker. • In a substudy amiodarone did increase the DFT by 1.29J. 4
recommendations • Most of these studies have been carried out in pts with ICDs for secondary prevention. • When medications are needed due to frequent shocks, optimising B Blocker therapy seems best initially. • How many shocks? Drugs are often not effective in pts with structurally normal hearts, channelopathies or acute MI and ablation may be very effective here in experienced centres. • If this is unsuccessful carefully individualised antiarrhythmic drugs may be added to lessen shocks and improve QoL. • Ablation techniques may be useful if drugs are unsuccessful. 4