Download
1 / 45
450 likes | 453 Views
Pharmacists as Medical Providers Credentialing and Privileging The Washington State Experience. Jeff Rochon , Pharm.D . Washington State Pharmacy Association. Learning Objectives. Explain Washington State SB 5557 and the ongoing implementation efforts.

E N D
Pharmacists as Medical ProvidersCredentialing and PrivilegingThe Washington State Experience Jeff Rochon, Pharm.D. Washington State Pharmacy Association
Learning Objectives • Explain Washington State SB 5557 and the ongoing implementation efforts. • Define credentialing and privileging for healthcare practitioners, including pharmacists. • Describe examples of pharmacist credentialing and privileging programs in the marketplace. • Explain the benefits of credentialing and privileging programs to advancement of pharmacists’ patient care delivery.
SB 5557 Highlights: Pharmacists as Patient Care Providers • Health plans recognize pharmacists as patient care providersfor covered benefits. • Health plans required to include adequate number of pharmacists in their participating provider networks. • Includes services covered as essential health benefits requirements. • Inclusion of pharmacies in health plans’ drug benefit networks do notsatisfy new requirements. • In short, pharmacists will be treated the same as other providers.
SB 5557 Highlights: Advisory Committee Process • OIC designated a lead organization. • Lead organization formed Advisory Committee. • Advisory Committee developed best practice recommendations for standards on credentialing, privileging, billing and payment • Advisory Committee provided best practice recommendations to OIC and DOH by December 1, 2015. • If needed, OIC and DOH develops rules based on recommendations.
Advisory Committee Work • INTENT: • To ensure that pharmacists will be regarded as any other provider, in accordance with relevant state law, as it relates to health plan billing, processing, and payment of claims for medical services that are provided. • SCOPE OF WORK: • Recommend guidelines for payment-dependent interactions between health plans and pharmacists/provider organizations, i.e. Contracting, Credentialing, Utilization Review, and Coding/Billing/Reimbursement.
Advisory Committee Deliverables Specific deliverables include: • FAQ document • Health Plan Policy Directives document • Pharmacists and Other Provider Expectations document
FAQ Document • Document reflects industry information, gathered during a discovery process that offers understanding and context for the recommended Policy Directives and Expectations. • Includes: • Clarifications about SB 5557 • Pharmacist’s scope of practice, licensure requirements, training, education, and certifications • Collaborative Drug Therapy Agreements (CDTA)
FAQ Document • What are Credentialing and Privileging and how do they apply? • Are pharmacists primary care providers or specialty care providers? Are there implications for co-pay? • What are the different places of service in which a pharmacist may practice? • Is a diagnosis required to bill for services? • What CPT/HCPCS Codes do pharmacists anticipate billing? How will they be reimbursed? • What are documentation and coding standards for medical services? • What claim forms are used for the billing of medical services? • Will Pharmacist bill directly or as “incident to”?
Are pharmacists primary care providers or specialty care providers? • For each of their benefit plans, the health plan (in withCMSand/ornationalmandates, e.g. ACA) willdetermineif a type of provider is to be designated as a primarycareprovider or a specialtycare provider.
Are there implications for patient co-pay? • YES. For somehealthplan productswhere a patient co-paydifferentialexists, thatdeterminationwillestablishwhetherthepatientwill have a primarycare co-pay or a specialtycare co-paywhenvisiting a provider ofthattype. ExplanatoryNote: 1. Whenmaking a "visit" to a provider, thepatientmay have a co-pay, theamountofwhich is determined by whetherthe provider visited is PrimaryCare or Specialty Care. 2. The co-pay is related to thevisitregardlessofthenumber and type of services delivered during thevisit. 3. The co-pay for an Emergency Room visit or a Hospital Admissionvisit is setregardlessofthenumber and types ofprovidersthatwilldeliver services over thecourseofthat ER or hospital visit.
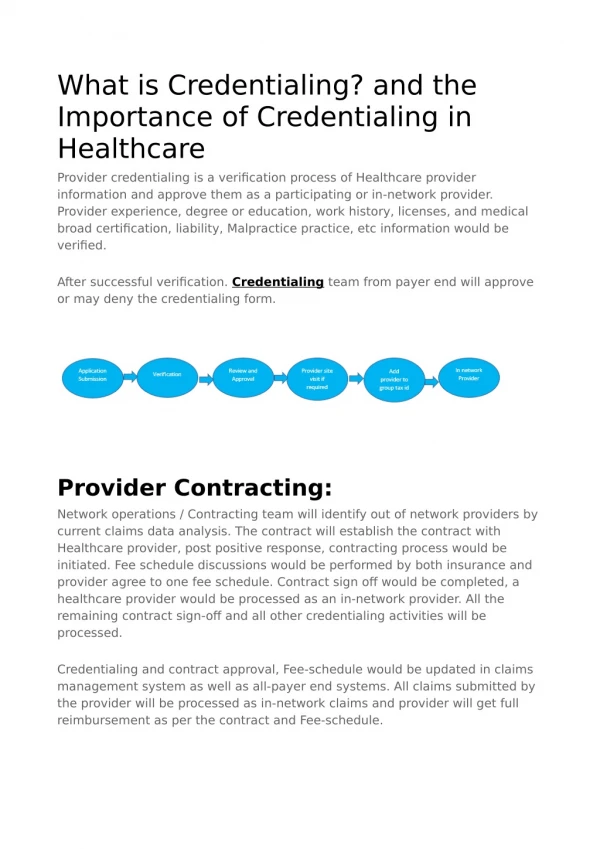
What is a Credential? • A credential is documented evidence of professional qualifications. • Such evidence includes: • Academic degrees, state licensure, residency certificates, training certificates, statements of continuing education (CE) credit, and board certifications. • Credentials are commonly earned within a professional domain (e.g., the license to practice a profession), but may also include evidence of individuals who have attained focused expertise in a particular disease state (certified diabetes educator, certified asthma educator, etc.)
Credentialing • Credentialing is a process that documents the attainment of qualifications to provide a scope of care expected Refers to one of two processes: 1) process of granting a credential designating that an individual has qualifications in a subject or area • e.g. granting a license or board certification to practice pharmacy 2) process by which a health plan, organization, or institution obtains, verifies, and assesses and individual’s qualifications to provide patient care services.
Credentialing • The processes for credentialing vary by institution and organization • Can be straightforward – simply verifying professional licensure and academic achievement • May be more complex – assessing the clinical experience and preparation for specialty practice beyond the assurances of professional licensure within a local organization.
Credentialing • Credentialing can be done via two major pathways: • Delegated credentialing is when a health plan has approved a provider organization’s process for defining, gathering and verifying a provider’s required set of credentials. • Direct credentialing is when a health plan or provider organization gathers and verifies the defined set of provider's credentials, and this process can require multiple months.
Delegated Credentialing • Some provider organizations have Delegated Credentialing Agreements with health plans allowing the provider organization to internally credential their providers. • When a provider organization performs ‘delegated credentialing’ on behalf of a health plan, the health plan approves the credentialing process already in place, which takes into account the health plan’s defined set of credentials as well as additional training and certification standards established within the provider organization. • In other words, the credentials required by the provider organization must meet, and can exceed, the set of credentials required by the health plan.
Direct Credentialing • Places responsibility on the individual provider to initiate the credentialing process with multiple health plans. • Process: • Starts with – Application from an individual • Verification – creates an applicant’s credential file Internal process or external verification process • Analysis – review and evaluation of the file • Decision – applicant notification • Ongoing monitoring, evaluation and improvement • Re-credentialing process initiated by applicant
The Credentialing Process • Am J Hlth-Syst Pharm, Vol 71, Nov. 1, 2014, p. 1893. Adapted from, Deutsch & Mobley, The Credentialing Handbook, Burlington, MA:Jones and Bartlett, 1999.
Council on Credentialing in Pharmacy (CCP) • The Council on Credentialing in Pharmacy (CCP) was established in 1999 to guide the professions credentialing programs • Supported by numerous pharmacy organizations • Resources available at: http://www.pharmacycredentialing.org/
What is a Certificate? • A certificate is a document issued to an individual when achieving a predetermined performance level
What are the currently recognized certifications a pharmacist can have? • The Council on Credentialing in Pharmacy has developed and maintains a list of pharmacist certifications • http://www.pharmacycredentialing.org/Files/CertificationPrograms.pdf • Certifications continue to evolve, so the list is not complete, but it is fairly comprehensive of the majority of certifications for pharmacists. • Currently there are no certifications available for many areas of pharmacy practice, e.g. reproductive health.
What is a privilege? • A privilege is permission or authorization granted by a hospital or other health care institution or facility to a health professional (e.g., physician, pharmacist, nurse practitioner) to render specific diagnostic, procedural, or therapeutic services. • Privileges are often different types: • Admitting privileges – giving the professional rights to admit patients • Clinical privileges – giving the professional rights to treat • Examples of privileges for pharmacists include pharmacokinetic dosing in hospitals, ordering labs, and monitoring/adjusting anticoagulants
Privileging • Privileging is the process by which a health care organization authorizes that individual to perform a specific scope of patient care services within that organization. • After reviewing the individual provider’s credentials and performance and finding them satisfactory • Authority is granted based on: • establishing that the provider has demonstrated competence to provide these services • the services are within the scope of provision of the organization • the organization can support their delivery. • Clinical privileges are both facility and individual specific
Privileging • As part of this privileging process, the credentials required of a provider, e.g. PA, ARNP, Pharmacist, may vary based on the specific services that a provider of that type delivers in the course of their work. • In other words, organizations may gather and verify different credentials of providers of a given type depending upon the services that the specific provider can/will deliver. • The determination of which credentials are required for which services is made using evidence-based standards that are reviewed by the organization’s medical staff and which is an integral part of the quality assurance review process.
Credentialing & Privileging Relationships • Are closely related processes • May occur in coordination • Both processes are designed to facilitate on-going quality improvement in individual performance using periodic peer-review • Providers must be willing to participate in quality improvement processes, and welcome the opportunity for peer assessment and support • The application of credentialing and privileging depends upon the type of organization.
Role of Health Plans • Health plans ONLY credential providers, i.e. they do not privilege providers. • For health plans, the defined set of credentials gathered and verified for a provider, e.g. PA, ARNP, Pharmacist, to deliver services to that health plan’s members do not vary based on the specific services that a provider of that type delivers in the course of their work.
Role of Provider Organizations • Provider organizations may credential only, or may credential AND privilege their providers. • Examples of these organizations include but are not limited to hospitals, ambulatory surgery centers, and medical clinics. • For provider organizations that privilege their providers: • the defined set of credentials gathered and verified for a provider, e.g. PA, ARNP, Pharmacist, may vary based on the specific services that a provider of that type delivers in the course of their work.
Role of Provider/Health Plan Organizations • Organizations that are both a provider organization AND a health plan • Provide patient care and take on financial risk for providing care • Examples of these organizations include but are not limited to Accountable Care Organizations (ACO), Health Maintenance Organizations (HMO), and Managed Care Organizations (MCO). • May credential only or may credential AND privilege their providers. • The defined set of credentials gathered and verified for a provider, e.g. PA, ARNP, Pharmacist, may vary based on the specific services that a provider of that type delivers in the course of their work. • These organizations have a baseline set of credentials that apply to all providers of a given type • AND they may have additional training and certification standards depending upon the services that the provider delivers.
Principles for Post-licensure Credentialing of Pharmacists • Based on a demonstrated patient/societal need • Established profession-wide through consensus • Credentialing programs should be accredited • Include measures to assess attainment of competencies • Enable pharmacists to obtain patient care privileges • Expect pharmacists to welcome peer-assessment of skills • Encourage employers & payers to adopt credentialing and privileging to authorize patient care responsibilities
Relationship to Reimbursement • Public expectation of competence underscores the authority to obtain payment for services • Quality improvement expectations hinge on willingness of providers to welcome peer-assessment and mentoring • Alignment with value-based performance measures (e.g. HEDIS, PQRS, Star Ratings, ACO measures, etc.) • Link to employer values and public reporting • Conditions of participation include payer authority for auditing of care provided • Should emulate medical credentialing (e.g. “resume-like” documentation), which is not skills assessment
Credentialing in Washington • Pharmacists will be credentialed either by • A health plan contracted organization, such as a facility or medical clinic, that performs health plan approved credentialing activities and has been approved for delegated credentialing, or • By completing an individual credentialing approval process with each health plan.
Credentialing in Washington As part of the credentialing process, every pharmacist must: 1. Demonstrate that they meet Washington State Pharmacy Licensure Requirements (RCW 18.64; WAC 246-861 and WAC 246-863)
Credentialing in Washington 2. Attest that all licensing requirements associated with services to be performed, including processes to obtain appropriate prescriptive authorization from healthcare provider(s) with independent prescriptive authority and/or appropriate CDTA(s), when applicable, have been/will be met. • Provide any/all CDTA identifier(s) that are on file with the PQAC. 3. Demonstrate that they have liability coverage at a minimum level established by the health plan, either independently or as part of a delegated or non-delegated group.
Credentialing in washington • It is recognized that a pharmacist’s education and training required for licensure meets the competency requirements for health plan covered services that fall within a pharmacist’s scope of practice. • Similar to other provider types, as service requirements become more advanced health plans may, at their individual discretion, require pharmacists to have advanced training and/or certification in addition to licensure in order to be considered for and subsequently be extended contracts within that Plan’s network.
Credentialing in Washington • When considering advanced training and certification requirements, health plans will take into account existing industry standard guidelines or recommendations. • This requirement may not be used in a manner designed to exclude categories of providers unreasonably (WAC 284-43-205(2)). • Health Plans are not required to guarantee that any specific licensed pharmacist will be included in their network.
Credentialing Process in Washington • In 2009, State Senate Bill 5346 was passed which includes a requirement that the Insurance Commissioner oversee the appointment of a private sector lead organization to manage the selection and implementation of a statewide provider database to collect and share information for credentialing, privileging and other uses. • The lead organization named was OneHealthPort. The vendor selected was Medversant and their application that collects provider data and allows the practice organization to manage all provider data is ProviderSource. The global service operated by OneHealthPort to manage sharing the data collected is called Provider Data Service.
Credentialing in Washington • While all health plans have their own processes for credentialing, ProviderSource within OneHealthPort is the new location from which all (or most) health plans should retrieve verified provider credentialing information.
Getting Started • In order to utilize OneHealthPort and ProviderSource, your organization must be registered. • This requires: • Choosing an Administrator – This is the person who will complete the registration process. • They must be authorized through their organization to agree to the terms and conditions of enrolling in OneHealthPort • OneHealthPort provides guidelines and responsibilities that can help organizations select their administrators • Completing the Registration Process • Creating Profiles for the Administrator and Organization • Sign Terms and Conditions Agreements • Verify Identity • Confirm Registration – Administrator will receive notification of organization and individual credential approval within 72 hours • Setup Secret Questions and Answers – for password self-resets as well as other security challenges required by some services
Getting Started • Once an organization is registered, the administrator can follow the OneHealthPort setup for ProviderSourceTM Users: A Step-By-Step Guidein order to: • Add additional administrators when necessary • Nominate providers/practitioners who will credentialed as a subscriber • This is how individual providers will be able to register and receive their login information
Registering Providers • To initiate the registration process for providers, an Administrator must nominate them • Completing nomination will automatically send the new subscriber a email and an activation code will be generated • The email includes the subscriber ID for the provider, next step instructions and a link to complete registration • *The activation code must be saved by the administrator sent separately to the provider • It is valid for 30 days from the time it was created
Registering Providers • To complete the registration process providers will need to: • Input their personal activation code • Complete the information request which includes full name, business contact information, date of birth, and gender • Create a password • Establish Security Questions • Once complete the provider will receive a confirmation message and can now login to access any OneHealthPort service or site.
Additional Step • For added security for sensitive provider information, a final step is required to apply “Browser Second Factor” security for ProviderSourceTM digital signature attestation of the practitioner record. • This online security feature provides additional protection to the provider’s login similar to most online banking sites. • The First time a provider logs in to a site that requires Second Factor level access they will need to answer the questions they set while making your password. • After answering the security questions a prompt will appear to name the provider’s device. • They will then be directed to the site they were trying to access
ProviderSource Credentialing • Providers should now be able to begin the credentialing process using the ProviderSource WPA field mapping template • The Introduction to ProviderSource video (located on the ProviderSource homepage) will help explain the basic functions of the application • Other helpful resources on the homepage include document uploading instructions and the electronic signature and attestation video
Health Plan Notification • In the Authorization and Release tab of the application, providers will be able to select which plans have access to their WPA after completion. • Some plans also require email notification when the application is complete. • In the right-hand column of the ProviderSource homepage is a link to notify plans • Fill out the required information and select the plans you want to notify and ProviderSource will send the form to the selected plans • Health plans accepting the form have agreed to respond within 7 days
Next Steps • The process and timeline after WPA completion and health plan notification can vary between plans • Providers can expect: • Notification that plans are reviewing completed WPA • The review process can vary from 30 days to 120 days • Notification of approval • Many plans provide approval notification by mailing copies of the provider’s contract that will need to be signed and returned