Download
1 / 138
1.5k likes | 2.08k Views
Heart. Pathology Department, Zhejiang University School of Medicine, Zhu keqing 竺可青, zhukeqing@yahoo.com , 2011-5-9. Atherosclerosis Coronary atherosclerosis/CHD Hypertension Aneurysm Rheumatism Infective endocarditis Chronic valvular vitium of the heart Cardiomyopathy

E N D
Heart Pathology Department, Zhejiang University School of Medicine, Zhu keqing 竺可青, zhukeqing@yahoo.com, 2011-5-9
Atherosclerosis Coronary atherosclerosis/CHD Hypertension Aneurysm Rheumatism Infective endocarditis Chronic valvular vitium of the heart Cardiomyopathy Myocarditis Pericarditis Congenital heart disease
Five categories of disease account for nearly all cardiac mortality • Congenital heart disease • Ischemic heart disease • Hypertensive heart disease (systemic and pulmonary) • Valvular heart disease • Nonischemic (primary) myocardial disease
Schematic representation of the sequence of events in cardiac hypertrophy and its progression to heart failure
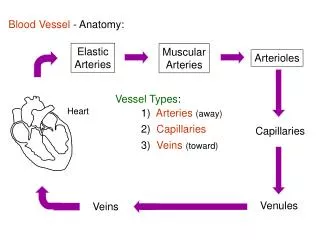
1. Atherosclerosis,AS • Arteriosclerosis动脉硬化: • Arteriolosclerosis 细动脉硬化 • Atherosclerosis(AS) • Medical calcification 动脉中层钙化 • 动脉硬化 • 指一组动脉壁增厚、变硬、弹性降低的疾病。包括动脉粥样硬化、动脉中膜钙化、细动脉硬化等。 • 动脉粥样硬化 • 指动脉内膜由于脂质沉积、胶原纤维和平滑肌增生、伴有坏死和钙化,引起动脉壁增厚变硬的疾病。主要侵犯大、中动脉
Risk factors for As 4高 • Hyperlipidemia • Hypertension • Smoking • DM(Diabetes mellitus) • Heritage • Age • Sex-Male • Lack of physical exercise • Obesity • Stress
Hyperlipidemia BAD GOOD • LDL/LDL-C HDL/HDL-C抗AS/CHD • sLDL—CHD • VLDL/CM乳糜微粒 • AS性脂蛋白表型—LDL(sLDL)\TG\VLDL\apoB异常升高与HDL-C/apoA-I降低
Endothelial cell response to environmental stimuli: causes (activators) and consequences (induced genes).
Schematic diagram of the mechanism of intimal thickening, emphasizing smooth muscle cell migration to, and proliferation and extracellular matrix elaboration in, the intima.
Evolution of arterial wall changes in the response to injury hypothesis
Schematic diagram of hypothetical sequence of cellular interactions in atherosclerosis
Theresponse to injury hypothesis(损伤应答学说), considers atherosclerosis to be a chronic inflammatory response of the arterial wall initiated by injury to the endothelium. • Moreover, lesion progression is sustained by interaction between modified lipoproteins(脂源性学说), monocyte-derived macrophages, T lymphocytes, and the normal cellular constituents of the arterial wall. • 脂质代谢障碍 • 高脂血症→脂蛋白(尤其β脂蛋白)↑→进入动脉内膜下沉积。 • 动脉内膜损伤 • 内膜通透性增高→脂蛋白进入增多 • 内膜损伤因素: • 1.高血压 • 2.吸烟 • 3.血管活性物质
Hypothetical sequence of cellular interactions in atherosclerosis • Chronic endothelial injury内皮细胞损伤, usually subtle, with resultant endothelial dysfunction, yielding increased permeability, leukocyte adhesion, and thrombotic potential Accumulation of lipoproteins, mainly LDL, with its high cholesterol content, in the vessel wall 血脂异常 • Modification of lesional lipoproteins by oxidation脂蛋白氧化修饰ox-LDL • Adhesion of blood monocytes (and other leukocytes) to the endothelium, followed by their migration into the intima and their transformation into macrophages and foamcells 泡沫细胞 • Adhesion of platelets血小板黏附 • Release of factors from activated platelets, macrophages, or vascular cells that cause migration of SMCs平滑肌细胞迁徙from media into the intima • Proliferation of smooth muscle cells in the intima, and elaboration of extracellular matrix, leading to the accumulation of collagen and proteoglycans • Enhanced accumulation of lipids both within cells (macrophages and SMCs) and extracellularly.
Morphology 脂纹脂斑期 肉眼:黄色斑点(帽针大)、黄色条纹。 镜检:泡沫细胞(单核细胞型、平滑肌细胞型) 纤维斑块期 肉眼:内膜表面灰黄色→瓷白色隆起斑块。 镜检:表层纤维帽、其下有平滑肌细胞、巨噬细胞、泡沫细胞和细胞外脂质(胆固醇)。 粥样斑块期 肉眼:表面斑块黄色或灰黄色,切面深层有粥糜样黄色物。 镜检:表层纤维帽;深层无定形坏死物,内有大量胆固醇;底部和边缘肉芽组织和少量泡沫细胞。 • The key processes in atherosclerosis are intimal thickening and lipid accumulation. • Fatty streak:foam cells 脂纹期---泡沫细胞 • Fibrous plaque: fibrous cap 纤维斑块(纤维帽) • Atheromatous plaque/atheroma 粥样斑块(粥瘤) • An atheroma粥瘤 consists of a raised focal lesion initiating within the intima, having a soft, yellow, grumous core of lipid (mainly cholesterol and cholesterol esters)胆固醇结晶, covered by a firm, white fibrous cap纤维帽.
American Heart Association classification of human atherosclerotic lesions from the fatty dot (type I) to the complicated type VI lesion
Schematic depiction of the major components of well-developed intimal atheromatous plaque overlying an intact media.
In the characteristic distribution of atherosclerotic plaques in humans the abdominal aorta腹主动脉瘤is usually much more involved than the thoracic aorta, • and lesions tend to be much more prominent around the origins (ostia) of major branches.
Atherosclerotic plaques have three principal components: • (1) cells, including SMCs, macrophages, and other leukocytes; • (2) ECM, including collagen, elastic fibers, and proteoglycans; • (3) intracellular and extracellular lipid. • These components occur in varying proportions and configurations in different lesions.
The advanced lesion并发症 of atherosclerosis: • 斑块破裂 Focal rupture, ulceration, or erosion of the luminal surface of atheromatous plaques may result in exposure of highly thrombogenic substances that induce thrombus formation or discharge of debris into the bloodstream, producing microemboli composed of lesion contents (cholesterol emboli or atheroemboli). • 斑块内出血 Hemorrhage into a plaque, especially in the coronary arteries, may be initiated by rupture of either the overlying fibrous cap or the thin-walled capillaries that vascularize the plaque. A contained hematoma may expand the plaque or induce plaque rupture. • 血栓形成 Superimposed thrombosis, the most feared complication, usually occurs on disrupted lesions (those with rupture, ulceration, erosion, or hemorrhage) and may partially or completely occlude the lumen. • 动脉瘤 Aneurysmal dilation may result from ATH-induced atrophy of the underlying media, with loss of elastic tissue, causing weakness and potential rupture. • 血管腔狭窄 • 钙化
View of the base of the brain, dissected to show the circle of Willis with an aneurysm of the anterior cerebral artery
Common sites of saccular (berry) aneurysms in the circle of Willis
Role of Acute Plaque Change.In most patients the myocardial ischemia underlying unstable angina, acute MI, and (in many cases) sudden cardiac death is precipitated by abrupt plaque change followed by thrombosis • Rupture/fissuring, exposing the highly thrombogenic plaque constituents. • Erosion/ulceration, exposing the thrombogenic subendothelial basement membrane to blood. • Hemorrhage into the atheroma, expanding its volume.
2 Coronary artherosclerosis(CAS) • 凡因冠状动脉狭窄造成心肌供血不足引起的心脏病,简称冠心病。以冠状动脉粥样硬化为最多见。 • 冠状动脉病CAD • 95%-99%CAS CAS=CAD CHD=IHD • 其余冠状动脉炎性疾病及畸形(风湿性/梅毒性主动脉炎)
Histologic features of atheromatous plaque in the coronary arteryA, Plaque rupture without superimposed thrombus, in patient who died suddenly. B, Acute coronary thrombosis superimposed on an atherosclerotic plaque with focal disruption of the fibrous cap, triggering fatal myocardial infarction. C, Massive plaque rupture with superimposed thrombus, also triggering a fatal myocardial infarction (special stain highlighting fibrin in red). In both A and B, an arrow points to the site of plaque rupture.
Estimated 10-year risk of coronary artery disease according to various combinations of risk factor levels
The clinical manifestations of IHD can be divided into four syndromes: 1 Myocardial infarction (MI), the most important form of IHD, in which the duration and severity of ischemia is sufficient to cause death of heart muscle. 2 Angina pectoris, in which the ischemia is less severe and does not cause death of cardiac muscle. Of the three variants--- stable angina, Prinzmetal angina, unstable angina-the latter is the most threatening as a frequent harbinger预兆 of MI. 3 Chronic IHD with heart failure. 4 Sudden cardiac death. • 冠心病的临床病理类型 • (1)心绞痛 • 冠状动脉供血相对不足,发生急性暂时性心肌缺血缺氧的临床综合征。 • (2)心肌梗死 • 冠状动脉供血绝对性不足,心肌持续性缺血缺氧,导致较大范围的心肌坏死。 • 发生原因: • ⑴冠状动脉粥样硬化合并血栓形成或斑块内出血。 • ⑵冠状动脉痉挛。 • ⑶在冠状动脉粥样硬化的基础上,由于过度负荷,造成心肌供血不足
Pathogenesis • The dominant influence in the causation of the IHD syndromes is diminished coronary perfusion relative to myocardial demand, • owing largely to a complex and dynamic interaction among: • fixed atherosclerotic narrowing of the epicardial coronary arteries, • intraluminal thrombosis overlying a disrupted atherosclerotic plaque, • platelet aggregation, • and vasospasm.
Atherosclerotic plaque rupture. A, Plaque rupture without superimposed thrombus, in patient who died suddenly. B, Acute coronary thrombosis superimposed on an atherosclerotic plaque with focal disruption of the fibrous cap, triggering fatal myocardial infarction.C, Massive plaque rupture with superimposed thrombus, also triggering a fatal myocardial infarction (special stain highlighting fibrin in red).
Schematic representation of sequential progression of coronary artery lesion morphology, beginning with stable chronic plaque responsible for typical angina and leading to the various acute coronary syndromes
Coronary Artery Pathology in Ischemic Heart Disease • Syndrome Stenoses Plaque Disruption Plaque-Associated Thrombus • Stable angina >75% No No • Unstable angina Variable Frequent Nonocclusive, often with thromboemboli • Transmural myocardial infarction FrequentOcclusive • Subendocardial myocardial infarction Variable Widely variable, may be absent, partial/complete, or lysed • Sudden death Usually severe Frequent small platelet aggregates / thrombi / thromboemboli
Angina pectoris • A symptom complex of IHD characterized by paroxysmal and usually recurrent attacks of substernal or precordial chest discomfort (variously described as constricting, squeezing, choking, or knifelike) caused by transient (15 seconds to 15 minutes)myocardial ischemia that falls short of inducing the cellular necrosis that defines infarction. • There are three overlapping patterns of angina pectoris: • (1) stable or typical angina, 稳定型 • (2) Prinzmetal or variant angina,变异型 • (3) unstable or crescendo angina. 不稳定型/恶化型
Stable angina The most common form and therefore called typical angina pectoris, appears to be caused by the reduction of coronary perfusion to a critical level by chronic stenosing coronary atherosclerosis.
Prinzmetal variant angina • An uncommon pattern of episodic angina that occurs at rest and is due to coronary artery spasm.
Unstableangina • Refers to a pattern of pain that occurs with progressively increasing frequency, is precipitated with progressively less effort, often occurs at rest休息, and tends to be of more prolonged duration. • In most patients, unstable angina is induced by disruption of an atherosclerotic plaque with superimposed partial (mural) thrombosis and possibly embolization or vasospasm (or both).
In the typical case of MI, the following sequence of events can be proposed: • The initial event is a sudden change in the morphology of an atheromatous plaque, that is, disruption-manifest as intraplaque hemorrhage, erosion or ulceration, or rupture or fissuring. • Exposed to subendothelial collagen and necrotic plaque contents, platelets undergo adhesion, aggregation, activation, and release of potent aggregators including thromboxane A2, serotonin, and platelet factors 3 and 4. • Vasospasm is stimulated by platelet aggregation and the release of mediators. • Other mediators activate the extrinsic pathway of coagulation, adding to the bulk of the thrombus. • Frequently within minutes, the thrombus evolves to completely occlude the lumen of the coronary vessel.
Postmortem angiogram showing the posterior aspect of the heart of a patient who died during the evolution of acute myocardial infarction, demonstrating total occlusion of the distal right coronary artery by an acute thrombus (arrow) and a large zone of myocardial hypoperfusion involving the posterior left and right ventricles.
The precise location, size, and specific morphologic features of an acute myocardial infarct depend on: • The location, severity, and rate of development of coronary atherosclerotic obstructions • The size of the vascular bed perfused by the obstructed vessels • The duration of the occlusion • The metabolic/oxygen needs of the myocardium at risk • The extent of collateral blood vessels • The presence, site, and severity of coronary arterial spasm • Other factors, such as alterations in blood pressure, heart rate, and cardiac rhythm.
冠状动脉粥样硬化:占95%最常见左前降支、其次右主干、再其次左旋支。斑块病变多发生于血管的心壁侧,呈新月形,使管腔呈偏心性狭窄。冠状动脉粥样硬化:占95%最常见左前降支、其次右主干、再其次左旋支。斑块病变多发生于血管的心壁侧,呈新月形,使管腔呈偏心性狭窄。 • 左前降支 Left anterior descending coronary artery (40% to 50%): infarct involves anterior wall of left ventricle near apex; anterior portion of ventricular septum; apex circumferentially • 右冠 Right coronary artery (30% to 40%): infarct involves inferior/posterior wall of left ventricle; posterior portion of ventricular septum; inferior/posterior right ventricular free wall in some cases • 左旋支 Left circumflex coronary artery (15% to 20%): infarct involves lateral wall of left ventricle except at apex
Schematic representation of the progression of myocardial necrosis after coronary artery occlusion • Subendocardial myocardial infarction 心内膜下心肌梗死 • Circumferential infarction 环状梗死 • Transmural myocardial infarction 透壁性心肌梗死
Acute myocardial infarct • 肉眼所见:梗死灶形状不规则呈地图状,其颜色随梗死时间而变化。梗死后6小时颜色苍白,9时土黄色,4天充血带,2-3周边红色,5周灰白色。 • 镜检:凝固性坏死,边缘充血和中性粒细胞浸润。
One-day-old infarct showing coagulative necrosis along with wavy fibers (elongated and narrow), compared with adjacent normal fibers (at right). Widened spaces between the dead fibers contain edema fluid and scattered neutrophils.
Dense polymorphonuclear leukocytic infiltrate in area of acute myocardial infarction of 3 to 4 days' duration
Nearly complete removal of necrotic myocytes by phagocytosis (approximately 7 to 10 days)
Granulation tissue characterized by loose collagen and abundant capillaries
Well-healed myocardial infarct with replacement of the necrotic fibers by dense collagenous scar