Download

1 / 105
1.05k likes | 1.5k Views
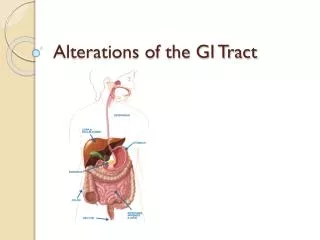
Nursing Care of Patients with Alterations in the GI tract. C. Cummings RN,EdD. A & P of GI system. GI tract. Hollow muscular tube, lumen surrounded by 4 tissue layers: Mucosa- innermost, thin layer of smooth muscle and exocrine cells Submucosa- connective tissue Muscularis- smooth muscle

E N D
Nursing Care of Patients with Alterations in the GI tract C. Cummings RN,EdD
GI tract • Hollow muscular tube, lumen surrounded by 4 tissue layers: • Mucosa- innermost, thin layer of smooth muscle and exocrine cells • Submucosa- connective tissue • Muscularis- smooth muscle • Serosa- outermost, connective tissue
GI tract • Function: • Secretion- secretes HCL acid, digestive enzymes • Digestion- mechanical and chemical, food is broken down to chyme • Absorption- from GI tract to blood supply • Motility • Elimination
GI tract • Nerve Supply • Intrinsic stimulation by myenteric plexus in smooth muscle and submucosa plexus in inner layer • Autonomic system- Parasympathetic stimulation by vagus nerve, connects with intrinsic system • Vagus-stimulates motor and secretory activity and relaxes spinchters • Sympathetic system- thoracic and lumbar splanchnic nerves slows movement, inhibits secretions and contracts spinchters
Mouth • Function: • Mastication, taste, begin movement • Glands produce 1 L of saliva/day • Saliva contains mucin and salivary amylase with begins to break down CHO • Oral preparatory phase- food is softened, made into a “bolus” and tongue moves to the back of the mouth • Oral phase- tongue presses bolus against hard palate, elevates the larynx and forces the food bolus to the pharynx, triggering swallowing • Pharyngeal phase- soft palate elevates and seals nasal cavity, inhibits respirations and allows esophagus to open • Esophageal phase- is when bolus enter at cricopharyngeal juncture, peristalsis now takes food to the stomach • All this takes about 10 seconds !
Esophagus • Canal about 10 in long, passes through the center of the diaphragm • Upper end is the upper esophageal sphincter, at rest it is closed to prevent air from entering the esophagus • Lower end is the lower esophageal sphincter, it sits at the gastroesophageal junction, at rest it is closed to prevent reflux of gastric contents, this is where GERD occurs • Function- to propel food and fluids and prevent reflux • Mucous is secreted to move the food along • Cardiac sphincter of the stomach opens to allow the food to enter
Stomach • Digestive and endocrine organ, in midline and LUQ • Four regions: • Cardia- narrow part that is distal to the gastroesophageal junction • Fundus- left above the GE junction • Body or corpus- largest area • Antrum- pylorus, is the distal portion and is separated from the duodenum by the pyloric sphincter, prevents backflow from the duodenum • Surface is covered in rugae or folds and have smooth muscle for motility • Has intrinsic and extrinsic nerves
Stomach • Function: • Parietal cells secrete HCL acid and intrinsic factor, which absorbs B 12, without it, what anemia can occur? • Chief cells secrete Pepsinogenpepsin • Cephalic phase- sight, smell and taste of food, regulated by vagus, begin secretory and contractile activity • Gastric phase- G cells in the antrum secrete gastrin, which causes HCL and pepsinogen to be released. HCL changes pepsinogen to pepsin, which digest proteins. Mucous and Bicarb are secreted to protect the stomach wall • Intestinal phase- chyme produced empties into the duodenum and causes distention, this produces secretin, which stops the acid production and gastric motility !
Small Intestine • Longest portion of the GI tract, 16-19 ft. • Made up of 3 sections: • Duodenum- first 12” and is attached to the pylorus. The CVD and pancreatic duct join to form the ampulla of Vater and empty into the duodenum at the duodenal papilla. This surrounded by a muscle, called the Sphincter of Oddi • Jejunum- middle 8 ft portion • Ileum- last 8-12 ft. The ileocecal valve separates the ileum form the cecum of the large intestine • Inner lining is made up of intestinal villi and folds of mucosa and submucosa for digestion.
Small Intestine • 3 main functions: • Movement- mixing and peristalsis • Moves chyme by segmental contractions and mixes with enzymes • Digestion- enzymes produced by the intestinal cells make: • Enterokinase, peptidases, lactase, maltase and sucrase • Help to digest, CHO, proteins and lipids • Absorption- absorbs most of the nutrients from food, takes 3-10 hours for the contents to pass through • Major organ for absorption
Large Intestine • Ileocecal valve to the anus, 5-6’, lined with columnar epithelium tha thas absorptive and mucous cells. • Cecum- is the beginning, dilated pouch like structure, appendix is attached to the base • Colon has 4 divisions: • Ascending, transverse, descending and sigmoid • Rectum- last 6-8” to the sphincter muscles and anus
Large Intestine • Function: • Movement- segmental contractions, to allow time for the water and electrolytes to be absorbed • Absorption- absorbs most of water and electrolytes, reduces fluid volume of chyme and creates a more solid mass for elimination • Elimination- 3-4 strong peristaltic contraction /day triggered by colonic distention in proximal large intestine to propel contents to rectum, until urge to defecate.
Nursing Assessment • Family history- GI disorders, cancer • Personal history- what kinds of things? • Diet history- anorexia, dyspepsia- what is that? What should you question them on for diet history? • Health history- diarrhea, constipation, # and color of stools, change in wt. or appetite • Abdominal pain- • P- precipitating • Q-quality- how intense, severe, type • R-region or radiation • S- severity scale- 0-10 • T-timing- when did it first occur, duration and frequency
Physical Assessment • Abdomen: • Inspection- skin, symmetry, rashes, lesions, scars • Auscultation- all four quadrants, normally heard in 5-15 seconds, normal, hypoactive or hyperactive, listen 1 full minute. What is borborygmus? Why would bruits be heard? Why would there not be bowel sounds heard? • Percussion- tympanic- air filled, dull- organ • Palpation- light and deep palpation, masses, tenderness, look for guarding
Lab tests • CBC- anemia • Oncofetal antigens- CA19-9 and CEA, used to monitor for cancer in the GI tract • Ca- decreased in malabsorption • K – decreased with vomiting, diarrhea • Xylose absorption- decreased indicates possible malabsorption in the small intesting • Stool for Occult blood • Stool for ova and parasite- infection • Stool for fecal fat- increased with Crohn’s disease and malabsorption
Radiology • Abdominal films- air in bowel and masses • Upper GI and small bowel- pharynx to duodenojejunal junction, barium swallow and SBFT • NPO 8 hours before, drink barium, then lie, stand and turn in multiple directions to view movement of barium • SBFT- drink more barium and view passage • After drink fluids to pass barium • Barium enema • Large intestine, done for obstructions, masses, not done is perforated colon or fistulas • Only clear liquids for 12-24 hours prior, NPO, given bowel prep like Golytely • Insert rectal catheter with a balloon and give 500-1500 ml of barium and hold • Can be uncomfortable, must take a laxative after
Diagnostic Tests • EGD- esophagogastroduodenoscopy • Visualize esophagus to duodenum, NPO prior, given versed and fentanyl, maybe cetacaine to inhibit gag reflex, pass tube and visualize structures, can take biopsies • Gag reflex may not return for 1-2 hours after, so no eating or drinking until then • Colonoscopy- large bowel, take biopsies and remove polyps, have a bowel prep prior, given versed and fentanyl prior; Capsule enteroscopy is now done to visualize, apply a data recorder to the abdomen and the patient swallows the capsule • Proctosigmoidoscopy- like colonoscopy, only a rigid tube, less invasive and does not require the cleansing of the colonoscopy
Case Study • 72 year old male admitted with chest pain and nausea. He states that he awakens in the night with pain in his chest and nausea. • What would you do first to evaluate his condition? • What diseases could he have? • What kind of lab work would you like to obtain? • What past medical history do you need?
Case Study • Your patient starts to have hematemesis. • What does this mean? • Is this life-threatening? • What interventions should be done? • What could have caused this condition?
Case Study • It is determined that your patient can be treated non-surgically. What medications would be given? (should have 3) • What type of teaching would be done for prevention? • If he needed surgery, what could have been done?
Esophageal Problems • GERD- gastroesophageal reflux disease • Reflux causes esophageal mucosa to be irritated by the effects of gastric and duodenal contents, results in inflammation • Causes: • Inappropriate relaxation of the LES, sphincter tone is decreased • Irritation from refluxed material • Delayed gastric emptying, gastric volume or intra-abdominal pressure is increased • Abnormal esophageal clearance
GERD • Refluxed material has a pH of 1.5-2, whereas the esophagus normally has a pH of 6-8 erosive esophagitis, once inflammed, the mucosa can’t eliminate the material as quickly. This leads to increased blood flow and more erosion. Gastric acid and Pepsin cause the tissue injury. • Can lead to Barrett’s epithelium- thicker, but can be cancerous, can also cause hemorrhage, aspiration pneumonia, asthma, laryngitis and dental deterioration.
GERD • Physical Manifestations: • Dyspepsia- heartburn, substernal or retrosternal burning that moves up and down in wavelike fashion, pain may radiate to neck or jaw or back, worsens when bends over, strains or lies on their back, occurs after meals and last 1-2 hours, helped by fluids and staying upright • Regurgitation- food entering throat without nausea, watch for cough, hoarseness or wheezing • Hypersalivation- water brash in response to reflux, fluid without sour or bitter taste
GERD • Physical Manifestations • Dysphagia and Odynophagia- difficulty swallowing, esophagus may be narrowed by inflammation or tumor, odynophagia- means what? • Chronic cough, mostly at night • Atypical chest pain • Belching and flatulence or bloating • Diagnosis: • Endoscopy, 24 hour ambulatory pH monitoring- pass a small tube into esophagus and monitor pH levels
GERD • Nursing Diagnoses: • What diagnoses would apply to these patients? • 1. • 2. • 3. • Interventions: • Diet therapy- what type of dietary modifications would be appropriate? • Certain foods decrease LES pressure- chocolate, fat and mints. Also, smoking and alcohol decrease • Spicy foods irritate the esophagus and Carbonated can increase gastric pressure
GERD • Lifestyle changes: • How should they sleep? • What things increase intra-abdominal pressure? • Drug therapy: • Goal is to inhibit gastric acid secretion, accelerate gastric emptying and protect the gastric mucosa • Antacids: • Elevate the pH and deactivate pepsin, good for heartburn, take 1 hour before and 2-3 hr after a meal • Name 2 antacids.
GERD • Drug therapy: • Histamine Receptor Antagonists • Decrease acid, help promote healing of the esophagus • Name 2 common ones sold OTC (generic ends in “dine”) • Proton Pump Inhibitors • Main treatment for GERD, long acting inhibition of gastric acid secretions by inhibiting protom pump of parietal cell, can reduce by 90%/ day • Name 2 proton pump inhibitors (generic ends in “zole”)
GERD • Other therapies: • Consider medications that may lower LES pressure- oral contraceptives, anticholinergics, sedative, tranquilizers, B-adrenergic agonists, nitrates and Ca channel blockers • Prokinetic drugs- for emptying and peristalsis- metoclopramide (reglan) • Endoscopic: • Enteryx procedure- spongy material in LES to tighten it Stretta procedure- radiofrequency energy through needles to inhibit the vagus nerve • Surgical: • Laparoscopic Nissen Fundoplication • Angelchik esophageal antireflux- anchors the LES in the abdomen to increase sphincter pressure
Hiatal Hernia • Protrusion of stomach through the esophagus • Sliding or Rolling hernias • Symptoms are similar to GERD patient • Nonsurgical management is like GERD • Surgical: • Lap Nissen Fundoplication- reinforces the LES, wraps a portion of the stomach around the distal esophagus to anchor it • Post op- risk for bleeding, infection and respiratory complications • Have an NGT, begin PO once BS return • Watch for gas-bloat syndrome and air swallowing
Nursing Diagnosis: GERD • Impaired Nutrition: less than body requirements • What things can be done to improve their intake and decrease pain? • What would be the expected outcomes? • How would you monitor their progress? • Acute Pain r/t irritation of the esophagus • What interventions can be performed? • Risk for aspiration r/t reflux of gastric contents • How can you determine that this does not occur?
Peptic Ulcer Disease • Mucosal lesion of the stomach or duodenum • Peptic can be gastric or duodenal • PUD- gastric mucosal defenses become impaired and they can no longer protect the epithelium from acid and pepsin • Three main types of ulcers: • Gastric • Duodenal • Stress
Gastric Ulcers • Gastric mucosa is protected by mucous and bicarbonate that maintain a normal pH on the gastric tissue and protects it from acid • Gastromucosal prostaglandins increase the barrier’s resistance to ulceration by producing mucous • Integrity is improved by a rich blood supply to the mucosa • If there is a break in the mucosal barrier, HCL acid damages the epithelium. Gastric ulcers result from back-diffusion of acid or dysfunction of the pyloric sphincter.
Gastric Ulcers • If the pyloric sphincter doesn’t function, bile backs up into the stomach, produces H+ ion back diffusion and mucosal inflammation • Toxic agents and bile destroy the lipid plasma membrane of the mucosa. Delayed gastric emptying also affects. What drug can be given to improve emptying? • Gastric Ulcers are deep and penetrating and usually are in the lesser curvature of the stomach, near the pylorus
Duodenal Ulcers • Occur in the first portion of the duodenum. • Deep lesions that penetrate through the mucosa and submucosa into the muscle layer. The floor of the ulcer consists of a necrotic area on granulation tissue and surrounded by fibrosis • High gastric acid secretion, pH levels are low for long periods • Protein rich meals, calcium and vagal excitation stimulate acid secretion • Hypersecretion, rapid emptying of food from stomach reduces the buffering effect of food and delivers a large acid bolus to the duodenum • Inhibitory secretory mechanisms and pancreatic secretion may be insufficient to control the acid • Many patients have H. pylori infection. H. pylori produces urease changes urea to ammonia, H+ ions released contribute to damage
Stress Ulcers • Acute gastric mucosal lesions occurring after and acute medical crisis or trauma • Associated with head injury, major surgery, burns, respiratory failure, shock and sepsis • Bleeding is the principle manifestation • Multifocal areas often in the proximal portion of the stomach and duodenum • Usually elevated HCL acid levels and hospital stay longer than 11 days
Complications of Ulcers • Hemorrhage: • 15-25% of patients with PUD, most serious complication • Most often with gastric ulcers and elderly • After initial bleed, 40% have a recurrence if untreated, especially if H. pylori untreated and no H2 antagonist • Have Hematemesis- bleeding at or above the duodenojejunal junction • Smaller amounts of bleeding are seen as melena, more often seen in duodenal ulcers, stool may appear black.
Complications of Ulcers • Perforation • Gastric or duodenal may perforate or bleed • Stomach or duodenal contents can leak into the abdomen, acid peptic juice, bile and pancreatic juice empty through the anterior wall of the stomach into the peritoneal cavity • Sudden, sharp pain in midepigastric region and spread over the abdomen • Amount of pain correlates with the amount and type of GI contents spilled • Abdomen is tender, rigid and boardlike, go into a fetal position to decrease tension of abdomen • Chemical peritonitis, bacterial septicemia and hypovolemic shock follow paralytic ileus and possible death