Download
1 / 20
200 likes | 229 Views
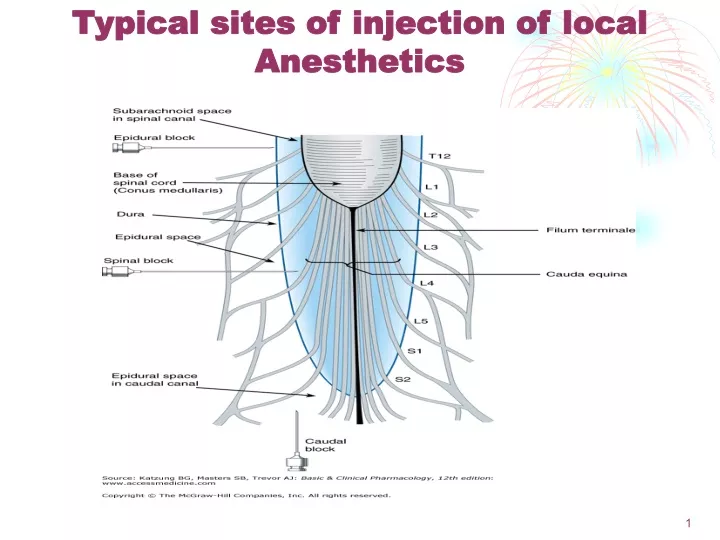
Typical sites of injection of local Anesthetics. 1. Differential Blockade : C---- B ----- A Autonomic Pain Cold Warmth Touch Pressure Motor. 2. Pharmacokinetic Properties of LA. Absorption and Distribution depends on : Dose Vascularity Physicochemical Properties pH

E N D
Differential Blockade: • C---- B ----- A • Autonomic • Pain • Cold • Warmth • Touch • Pressure • Motor 2
Pharmacokinetic Properties of LA Absorption and Distribution depends on : • Dose • Vascularity • Physicochemical Properties • pH Metabolism includes : • The metabolic degradation of local anesthetics depends on whether the compound has an ester or an amide • Esters are extensively and rapidly metabolized in plasma by pseudocholinesterase • the amide linkage is resistant to hydrolysis • In patients with atypical plasma cholinesterase, the use of ester linked compounds, such as chloroprocaine, procaine and tetracaine, has an increased potential for toxicity. • The hydrolysis of all ester-linked local anesthetics leads to the formation of paraaminobenzoic acid (PABA), which is known to be allergenic • Local anesthetics with an amide linkage (and one ester-lined anesthetic, cocaine) are almost completely metabolized by the liver before excretion. 3
Pharmacological and Toxicological Effects of LA Cardiac Effects: decreased excitability and contractility. Vascular Effects: usually vasodilation which will reduce venous return and consequently cardiac output. Central Effects: can cross BBB due to small size. Usually produce CNS stimulation. CNS depression occurs with high doses Neuromuscular & Ganglia: can decrease ACh release. Hypersensitivity Reactions:. Usually with esters. Might also be due to the preservatives . 1/1/2020 4
Topical LA Agents skin graft is a surgical operation in which a piece of healthy skin is transplanted to a new site on a patient's body or to a different individual. • EMLA: • “Eutectic (سهل الانصهار)Mixture of Local Anesthetics” • For children to reduce the pain of venipuncture. • TAC: • Tetracaine + Adrenaline + Cocaine. • For skin graft 1/1/2020 5
General Anesthesia Definition: Loss of memory, awareness and pain sensation during a surgical procedure, together with loss of reflexes, and skeletal muscle relaxation.
Features of an Ideal General Anesthetic Rapid loss of awareness and memory. Analgesia limiting reflexes. Minimal and reversible influence on vital signs. Skeletal muscle relaxation. Operating room safety. Rapid emergence or recovery. Balanced Anesthesia: Multi drug approach to manage the patient’s anesthetic needs. Phases of Anesthesia • Induction • Maintenance • Emergence = Recovery
Stages of Anesthesia Classically Described for Ether Anesthesia: . Stage I: “ Analgesia” Amnesia and euphoria. is the period between the initial administration of the induction agents and loss of consciousness . Stage II: “Excitement” Delirium and combative behavior. the period following loss of consciousness and marked by excited and delirious activity. During this stage, respirations and heart rate may become irregular. In addition, there may be uncontrolled movements, vomiting, breath holding, and pupillary dilation. . Stage III: “Surgical Anesthesia” Anesthesia, regular respiration and decreasing eye movements. . Stage IV: “Medullary Depression” Respiratory and cardiac depression and arrest and no eye movements. the most common use of ethers has been in anesthesiology. Diethyl ether has the unfortunate disadvantage of being extremely flammable, especially in the presence of enriched oxygen mixtures. This property has resulted in many instances of fires in operating rooms during surgery amnesia is loss of memory.
Preanesthetic Medications" Premedication" • Opioids • Benzodiazepines • Antimuscarinics • Antihistamines • Antiemetics
Intravenous Anesthesia induce anesthesia within one or two circulation times after their administration because they rapidly achieve initial high concentration in the (CNS). Very lipid soluble so they enter the brain. Very short t½. The rate of initial redistribution following the administration of a single IV bolus of drug is defined by the half-life (t1/2) Tissues with lower blood flow per unit mass will receive and therefore remove proportionally less anesthetic during the initial phase of drug distribution. The use of IV anesthetics permits the patient to pass rapidly through the initial stages of anesthesia, and sleep is induced quickly
Most of the IV drugs used to induce anesthesia are slowly metabolized and excreted and depend on redistribution to terminate their pharmacological effects • Tissues with an intermediate blood flow per unit of mass, such as skeletal muscle and skin, are among the first to participate in drug redistribution. In fact, it is the patient’s skeletal muscle tissue groups that will contain the largest proportion of the initial dose of anesthetic when the patient awakens • Repeated administration leads to delayed awakening. • Computer assisted i.v. administration (Total Intravenous Anesthesia TIVA). • Fat tissue, and bone require hours to come into equilibrium • with plasma drug concentrations. Since the accumulation of anesthetic in body fat is relatively small soon after its IV administration, it is common clinical practice to calculate drug dosage on the basis of lean body mass rather than on total body weight. Thus, an obese patient may receive the same dose of IV anesthetic as a patient of normal body weight.
The distribution of thiopental in body tissues and organs following intravenous injection. Note the redistribution of the drug, with time, to tissues with lower rates of blood flow. Intravenous Anesthesia General Uses: Ideally suitable for Induction. Maintenance of short procedures. Supplement inhalational anesthesia.
INTRAVENOUS ANESTHETIC AGENTSUltra Short Acting Barbiturates Thiopental ------- most popular i.v. agent for induction Methohexital -------- very short acting, Weak acids, can precipitate . Patients may react to painful stimuli but: Unaware, Do not remember. Cardiorespiratory depressants Benzodiazepines • Diazepam --- viscous formulation so can precipitate. • Midazolam --- aqueous , t½ 2hrs. • Lorazepam --- long t½, viscous. • All do not depress cardiorespiratory function. • Flumazenil, is the antidote for overdose. acts by binding CNS benzodiazepine receptors and competitively blocking benzodiazepine activation of inhibitory GABAergic synapses.
Ketamine Dissociative Anesthesia: Profound analgesia, amnesia and superficial sleep. Patient appears awake and reactive but does not respond to sensory stimuli. Blocks glutamic acid at NMDA receptor Given for Children by IM injection And Ambulatory conditions ---used in military. used mainly for starting and maintaining anesthesia. Other uses include sedation in intensive care, as a pain killer, as treatment of bronchospasm, as a treatment for complex regional pain syndrome and as an antidepressant The N-methyl-D-aspartate receptor (also known as the NMDA receptor or NMDAR), is a glutamate receptor and ion channel protein found in nerve cells • Catatonia(جامود ): a state of apparent unresponsiveness to external stimuli in a person who is apparently awake, with mild increase in muscle tone, eyes opened and nystagmus(رأرأة العين). • Maintains cardiovascular function. • May evoke excitatory and hallucinatory phenomena during emergence, so needs a quiet recovery room. • Might also cause shivering, tachycardia, increased intracranial and intraocular pressures.
Propofol Propofol (Diprivan) is rapidly acting, has a short recovery time, and possesses antiemetic properties Most popular IV anesthetic, replaced thiopental. Propofol lacks analgesic properties, its use permits lower doses of opioids ICU patients: prolonged sedation Produces euphoria--- good for induction. Anti-emetic, better postoperative period. Pain at site of injection, muscle tremors. Rapidly metabolized
Narcotics originally referred medically to any psychoactive compound with any sleep-inducing properties. In the United States it has since become associated with opiates and opioids Suitable for cardiac surgery. Not good amnesics. Continuous infusion will depress ventilation. Morphine ----- lowers BP , Bronchospasm Meperidine ----- Increases -HR Fentanyl Sufentanil Alfentanil Remifentanil.
Chemical structures of intravenous anesthetics. Half-life time of common intravenous anesthetics Half-life (t1⁄2) is the amount of time required for the amount of something to fall to half its initial value
Inhalational Anesthesia The inhalational anesthetics can be divided into two classes based on their physical properties. N2O and cyclopropane are gases at room temperature and are supplied in gas tanks that are regulated by the anesthesia machine. Gases or Volatile Liquids Elimination is by the lungs Metabolism is slow Equilibration with tissues. Interaction with tissues and liquids is physical.
Inhalational Anesthesia Since the anesthesiologist has control over the partial pressure of anesthetic delivered to the lung, it can be manipulated to control the anesthetic gas concentration in the brain, hence the level of unconsciousness Anesthetic dose is usually expressed in terms of the alveolar tension required at equilibrium to produce a defined depth of anesthesia. The dose is determined experimentally as the partial pressure needed to eliminate movement in 50% of patients challenged with a standardized skin incision.
Inhalational Anesthesia the minimum alveolar concentration (MAC) is usually expressed based on the percentage of inhaled gases that is represented by anesthetic gas at 1 atm Anesthetic delivery involves Delivering System Alveoli Blood -------- CNS Tissues