Download
1 / 36
390 likes | 726 Views
Erythema Nodosum. Basic Dermatology Curriculum. Last updated March 23, 2011. Modules Instructions.

E N D
Erythema Nodosum Basic Dermatology Curriculum Last updated March 23, 2011
Modules Instructions • The following module contains a number of blue, underlined terms which are hyperlinked to the dermatology glossary, an illustrated interactive guide to clinical dermatology and dermatopathology. • We encourage the learner to read all the hyperlinked information.
Goals and Objectives • The purpose of this module is to help medical students develop a clinical approach to the evaluation and initial management of patients presenting with erythema nodosum. • By completing this module, the learner will be able to: • Identify and describe the morphology of erythema nodosum • Name conditions associated with erythema nodosum • Recommend an initial treatment plan for a patient with erythema nodosum • Discuss when to refer to a patient with erythema nodosum to a dermatologist
Case One Mrs. Cheryl Mosely
Case One: History • HPI: Mrs. Mosely is a 35-year-old woman who presents to her primary care physician with tender red “bumps” on her anterior shins. The lesions appeared over the course of a few days and have started to resolve with faint bruises remaining. She also reports a recent history of a sore throat and fever two weeks ago, which improved after a course of antibiotics. • PMH: no major illness or hospitalizations • Medications: none aside from recent antibiotic course • Allergies: none • Family history: noncontributory • Social history: lives with husband and 12-year-old child who also had a sore throat • Health-related behaviors: no tobacco, alcohol, or drug use • ROS: no cough or rhinorrhea
Case One: Exam • Vital signs: normal • Gen: well-appearing • HEENT: normal • Skin: multiple scattered shiny, red nodules on the anterior shins bilaterally
Case One, Question 1 • What is the appropriate next step? • Anti-Streptolysin O titer • Biopsy the lesion • Drain the nodules • Topical steroid ointment
Case One, Question 1 Answer: a • What is the appropriate next step? • Anti-Streptolysin O titer • Biopsy the lesion (diagnosis can be made clinically) • Drain the nodules (lesions are more inflammatory vs. abscess) • Topical steroid (not effective)
Diagnosis: Erythema Nodosum • Mrs. Mosely’s recent history of sore throat and fever is suggestive of acute pharyngitis. Her ASO titer came back elevated. • The lesions on her legs were diagnosed as erythema nodosum.
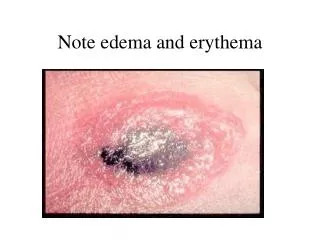
Erythema Nodosum (EN) • Characterized by the presence of painful, erythematous, non-ulcerative nodules • Often symmetric distribution, located bilaterally below the knees (mainly on the anterior tibial surface) • Lesions evolve from bright red to brown-yellow, resembling old ecchymoses • Old and new lesions often coexist • Patients may also present with fever, fatigue, and arthralgias • The morphology of the lesion, a deep nodule, identifies EN as an inflammatory disease of the fat (called a panniculitis)
Case One, Question 2 • Which of the following history and clinical items are commonly found in patients with EN? • Patient is female • Recent fever • Recent upper respiratory infection • Use of oral contraceptives • All of the above
Case One, Question 2 Answer: e • Which of the following history and clinical items are commonly found in patients with EN? • Patient is female • Recent fever • Recent upper respiratory infection • Use of oral contraceptives • All of the above
EN: The Basics • Can occur at any age, but most cases appear between 2nd and 4th decades • 15-20x more common in women than men • EN is not a disease, but a reaction pattern to a variety of factors including infections, medications, and systemic diseases • Diagnosis of EN should always be followed by a search for the underlying etiology • Streptococcal disease is the most common cause of EN in children • Drugs, sarcoidosis, and inflammatory bowel disease (IBD) are commonly associated disorders in adults with EN
Conditions Associated with EN • Idiopathic > 50% • Infections • Streptococcal infections, tuberculosis, histoplasmosis, coccidiomycosis • Drugs • Oral contraceptive pills, sulfonamides • Neoplasms • Lymphoma, leukemia, renal cell carcinoma • Miscellaneous Conditions • Sarcoidosis, inflammatory bowel disease Note: Only a few common causes of EN are mentioned. EN is associated with a wide variety of disease processes and medications.
Case One, Question 3 • Which of the following statement regarding treatment of EN is true? • Antihistamines are often used for treatment • Anti-inflammatories should be avoided • EN tends to be self-limited • Systemic steroids are of no value
Case One, Question 3 Answer: c • Which of the following statement regarding treatment of EN is true? • Antihistamines are often used for treatment (Not true) • Anti-inflammatories should be avoided (Not true. Anti-inflammatories are often used in the treatment of EN) • EN tends to be self-limited • Systemic steroids are of no value (Not true. Systemic steroids can be used if underlying infection and malignancy have been excluded)
EN: Treatment • EN is usually self-limited or resolves with treatment of the underlying disorder • Lesions heal without atrophy or scarring • Eruption generally lasts from 3 to 6 weeks, and recurrences are frequent • Treatment is typically symptomatic • Supportive measures and pain control are recommended • The use of systemic glucocorticoids should be weighed against the possibility of masking an underlying neoplastic, inflammatory, or infectious condition • Oral potassium iodide therapy is another treatment option
Case Two Ms. Beverly Prescott
Case Two: History • HPI: Ms. Prescott is a 35-year-old woman who presents to her primary care provider with tender red nodules on her anterior shins. Some of the lesions appear to be resolving, but others are still appearing. No sick contacts or anyone else with a rash. • PMH: no major illnesses or hospitalizations • Allergies: none • Meds: oral contraceptive pills (unable to recall the name) • Family history: father with history of BCC • Social history: lives with a friend in an apartment, works in advertising • Health-related behaviors: alcohol use (1-2 drinks per week), no tobacco or drug use • ROS: negative
Case Two: Exam • Vital Signs: normal • HEENT: normal exam • Lungs: clear to auscultation • Skin: multiple scattered shiny, erythematous nodules on the anterior lower extremities
Case Two, Question 1 • The primary care provider suspects erythema nodosum. What else should be considered as part of the initial evaluation? • Make sure a thorough medical history and review of systems was performed • Order an ASO • Place a PPD • All of the above
Case Two, Question 1 Answer: d The primary care provider suspects erythema nodosum. What else should be considered as part of the initial evaluation? Make sure a thorough medical history and review of systems was performed Order an ASO Place a PPD All of the above
Case Two, Question 2 • What is the likely cause of Ms. Prescott’s erythema nodosum? • Crohn’s disease • Oral contraceptives • Sarcoidosis • Tuberculosis
Case Two, Question 2 Answer: b What is the likely cause of the Ms. Prescott’s erythema nodosum? Crohn’s disease (Possible that EN is the presenting feature of IBD, but her OCP use is a more likely cause in this case) Oral contraceptives Sarcoidosis (Possible, but less likely) Tuberculosis (No known risk factors, but a PPD placement would be prudent)
Case Three Ms. Maria Ojeda
Case Three: History • HPI: Ms. Ojeda is a 50-year-old woman who presents to the general medicine clinic with tender red nodules on her posterior calves for the past 2 months. • PMH: last visit to the doctor was 10 years ago, no major illnesses or hospitalizations • Medications: none • Allergies: none • Family history: mother with hypertension • Social history: lives with multiple family members in the city, recently moved to the US from Guatemala • Health-related behaviors: no tobacco, alcohol, or drug use • ROS: occasional fatigue
Case Three: Exam • Vital signs: normal • Physical exam normal except for: tender erythematous shiny nodules on the posterior calves bilaterally
Case Three, Question 1 • What is the most likely diagnosis? • Erythema induratum • Erythema nodosum • Polyarteritis nodosa • Syphilitic gumma
Case Three, Question 1 Answer: a What is the most likely diagnosis? Erythema induratum Erythema nodosum (Characterized by painful, erythematous, non-ulcerative nodules usually located on anterior lower legs) Polyarteritis nodosa (Characterized by painful, subcutaneous nodules. Livedo reticularis may be present) Syphilitic gumma (Painless subcutaneous nodules, enlarge, attach to the overlying skin, and eventually ulcerate)
Erythema Induratum • Erythema induratum is a panniculitis characterized by tender subcutaneous nodules usually located on the lower posterior calf • Erythema induratum is chronic and more commonly affects middle-aged women • Occurs in the setting of tuberculosis (latent) • PPD will usually be positive • Lesions can resolve spontaneously with or without ulceration and often heal with scarring
When to Biopsy Panniculitis • For persistent lesions (> 6wks) or when the diagnosis is unclear a biopsy is typically necessary and these patients should be referred to a dermatologist • A deep incisional or excisional biopsy should be obtained for best visualization because a punch biopsy is likely to produce an inadequate sample
Take Home Points • EN is characterized by painful, erythematous, non-ulcerative subcutaneous nodules. • Most cases appear between the 2nd and 4th decade of life and is more common in women. • There are numerous etiologies for EN including infections, medications, neoplasms, and other miscellaneous conditions. • Streptococcal infection is the most common etiologic factor in children.
Take Home Points • Drugs, sarcoidosis, systemic fungal infections (coccidiomycosis, histoplasmosis) and inflammatory bowel disease are commonly associated disorders in adults with EN. • EN tends to be self-limited or resolves with treatment of the underlying disorder. • Erythema induratum can be distinguished from EN by the chronic time course, location on the posterior calf, ulceration of the lesions and association with latent tuberculosis.
Acknowledgements • This module was developed by the American Academy of Dermatology Medical Student Core Curriculum Workgroup from 2008-2012. • Primary authors: Sarah D. Cipriano, MD, MPH; Eric Meinhardt, MD; Timothy G. Berger, MD, FAAD. • Peer reviewers: Peter A. Lio, MD, FAAD; Carlos Garcia, MD. • Revisions and editing: Sarah D. Cipriano, MD, MPH; Jillian W. Wong. Last revised March 2011.
End of the Module • Berger T, Hong J, Saeed S, Colaco S, Tsang M, Kasper R. The Web-Based Illustrated Clinical Dermatology Glossary. MedEdPORTAL; 2007. Available from: www.mededportal.org/publication/462. • Bolognia Jean L, Braverman Irwin M, "Chapter 54. Skin Manifestations of Internal Disease" (Chapter). Fauci AS, Braunwald E, Kasper DL, Hauser SL, Longo DL, Jameson JL, Loscalzo J: Harrison's Principles of Internal Medicine, 17e: http://www.accessmedicine.com/content.aspx?aID=2864525. • James WD, Berger TG, Elston DM, “Chapter 16. Mycobacterial Disease” (chapter). Andrews’ Diseases of the Skin Clinical Dermatology. 10th ed. Philadelphia, Pa: Saunders Elsevier; 2006: 337. • James WD, Berger TG, Elston DM, “Chapter 23. Diseases of Subcutaneous Fat” (chapter). Andrews’ Diseases of the Skin Clinical Dermatology. 10th ed. Philadelphia, Pa: Saunders Elsevier; 2006: 487-489.
End of the Module • Requena L, Yuz ES. Erythema Nodosum. Semin Cutan Med Surg. 2007;26:114-125. Requena Luis, Yus Evaristo S, Kutzner Heinz, "Chapter 68. Panniculitis" (Chapter). Wolff K, Goldsmith LA, Katz SI, Gilchrest B, Paller AS, Leffell DJ: Fitzpatrick's Dermatology in General Medicine, 7e: http://www.accessmedicine.com/content.aspx?aID=2978288. • Schwartz RA, Nervi SJ. Erythema Nodosum: A Sign of Systemic Disease. Am Fam Physician. 2007;75:695-700. • Wolff K, Johnson RA, "Section 7. Miscellaneous Inflammatory Disorders" (Chapter). Wolff K, Johnson RA: Fitzpatrick's Color Atlas & Synopsis of Clinical Dermatology, 6e: http://www.accessmedicine.com/content.aspx?aID=5201183.