Download
1 / 49
500 likes | 762 Views
Rh Discrepancies in Prenatal Patients -A Practical Approach to Management. CBS TM Resident Session September 15 th , 2009 Dr. Judith Hannon Dr. Gwen Clarke. Rh genetics… a brief review. Rh genetics. RHD and RHCE. 2 RH Genes RHCE and RHD on Chromosome 1; 10 exons each

E N D
Rh Discrepancies in Prenatal Patients-A Practical Approach to Management CBS TM Resident Session September 15th, 2009 Dr. Judith Hannon Dr. Gwen Clarke
Rh genetics… a brief review Rhgenetics
RHD and RHCE 2 RH Genes RHCE and RHD on Chromosome 1; 10 exons each D and CE vary at only 32 -35 amino acid positions (or are 97% identical) C/c and E/e encoded by RHCE
Rh Genetics www.uni-ulm.de/~wflegel/RH/
D negative Deletion of RHD due to unequal crossover between upstream and downstream genetic elements (15 – 17% in caucasians) RHD with 37bp internal duplication and premature stop codon(66%) or hybrid RHD-CE-D with no D expression (15%) of Africans 10 – 30% of Asians with D negative serology are DEL and do express very low levels of D antigen; most arise from deletion or mutation in exon 9
Rh D and Rh CcEe Science.uwe.ac.uk
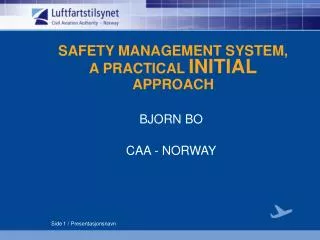
D positive but…Weak and partial D More than 100 D alleles identified by sequencing studies Weak D characterized by single or few aa changes primarily in transmembrane or cytoplasmic part of D protein; 0.2 – 1% of Caucasians; may react weakly or not at all in direct agglutination assays Partial D characterized by aa changes in the extracellular portions of D polypeptide; type as D positive with some antisera
Weak and partial D Blood, Vol. 93, Issue 1, 385-393, January 1, 1999Wagner, Gassner, Muller, et al
How often does this happen? Weak D: 0.2 – 1% of Caucasian population Types 1, 2 and 3 represent >90% of these These types are NOT immunized to make anti D Partial D: Most react strongly with most anti D reagents May present when they make anti D Most that make anti D are DVI representing 0.02 – 0.05% of population
Anti D anti Sera Monoclonal anti D Antibody directed against a single epitope of the D antigen Produced in vitro from a cell line (recombinant) expressing a particular immunoglobulin gene sequence Several monoclonals may be “blended” Polyclonal anti D A group of anti D antibodies directed against a variety of epitopes on the protein; naturally occurring following an immune response to D immunization.
Anti Sera reactivity Varies with combination and number of epitopes detected by a particular reagent Blended monoclonals have broad reactivity with most weak and partial D and produce strong reactions. Limited specificity monoclonals react with fewer epitopes and react with only some examples of partial D
Rh D and Rh CcEe Science.uwe.ac.uk
Reaction strength and phase In general, D positive individuals have strongly agglutinated cells in the presence of anti D (3 – 4+) Repeated 1 – 2+ reactivity may indicate weak or partial D status Weak D testing – or testing at the IAT phase will result in almost all weak and partial D’s typing as D positive – including DVI individuals.
Commercially available anti D antisera in Canada Monoclonal Novaclone IgM IgG Bioclone ANTI D Monoclonal blend ANTI D Monoclonal IgM Immucor Series 4 Monoclonal Blend Immucor Series 5 Monoclonal Blend Polyclonal Olympus (for PK7300) Immucor Seraclone Biotest Anti D
Development of an Algorithm to Resolve Serological RhD Typing Discrepancies Post-Galileo Implementation in the Prenatal Laboratory
Background • March 2006- CBS discontinued weak D testing of prenatal patients (moms) in keeping with international practises. • May 2006 – Immucor GalileoTM replaced Olympus PK7200 in CBS Prenatal Testing Laboratory, Edmonton. • Required reagent change from Novaclone to Immucor Series 4 (S4) and Series 5 (S5) anti-D. • Validation included parallel testing for 3 days (673 samples) with 100% concordance for RhD results.
RhD Discrepancies • May 31, 2006, 1st patient identified who had previously tested RhD POS (Olympus PK7200 – Jan 2005) and was now testing RhD NEG on Galileo (Immucor S4 and S5 anti-D) - Rh Inconclusive. Manual Tube (IS): Immucor S4 w+ micro Immucor S5 NEG DBL Novaclone 2+ Gammaclone 2+ • Sample sent to Mount Sinai Hospital in Toronto for molecular testing- wk D Type 1 allele- known not to form anti-D- report amended to RhD positive. • Cause of discrepant results? Reagent specificity? Method? (incubation time or temperature)
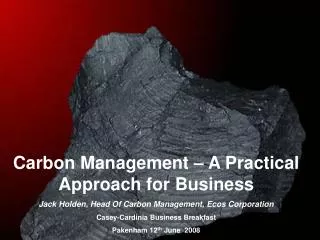
Molecular Testing • May 2006 to Dec 31, 2006 – discrepant samples retested with manual tube technique using antisera panel (S4, S5, Novaclone, Gammaclone). RhD status assigned based on serological testing. • Hospitals were receiving discrepant results and CBS was finding discrepancies with previous test records, both prenatal and XM. • Reporting results as Rh inconclusive compromised the ability of hospitals to use an electronic X-match which is in widespread use in Alberta. • Jan 1, 2007 to Apr 14, 2008 all RhD discrepant samples sent to Mount Sinai Hospital Molecular Testing Laboratory on a study basis (Dr. Greg Denomme) • Total samples screened on Galileo = 88,972. Total discrepant samples sent for DNA analysis = 209 (0.23% of total)
Molecular Testing of Prenatal RhD Typing Discrepancies Following Galileo Total Tested = 88 972 Total discrepancies sent for DNA typing=209 (0.23% of total)
Based on data from molecular testing an algorithm was proposed for assigning RhD status to patients with discrepant results on serological testing • At least 1 Galileo anti-D score ≤ 1+ prompted standardized tube tests with S4 and S5 • If tube tests agreed & < 2+ →Rh NEG • If tube tests agreed & ≥ 2+ →Rh POS • If tube tests did not agree (with ≥ 2+ difference between reagents) →Molecular testing
Examples of Discrepant Results – WD Types 1 & 2 (NOT AT RISK) At least 1 Galileo Score ≤ 1 → Tube Tests (S4, S5) Tube Tests Agree ≥ 2+ Rh POS Tube Tests Agree < 2+ Rh NEG Tube Tests Disagree (2+ diff) MOLECULAR Testing
Examples of Discrepant Results – WD Types 3 & 4 (NOT AT RISK) At least 1 Galileo Score ≤ 1 → Tube Tests (S4, S5) Tube Tests Agree ≥ 2+ Rh POS Tube Tests Agree < 2+ Rh NEG Tube Tests Disagree (2+ diff) MOLECULAR Testing
Examples of Discrepant Test ResultsUnclassified, DAR, DVI (AT RISK) At least 1 Galileo Score ≤ 1 → Tube Tests (S4, S5) Tube Tests Agree ≥ 2+ Rh POS Tube Tests Agree < 2+ Rh NEG Tube Tests Disagree (2+ diff) MOLECULAR Testing
Using the Proposed Algorithm Results of Previous Molecular Testing were Analyzed
Problem! • 97% of individuals classified as Rh NEG using algorithm were WDT 1, 2, 3 and 4 and did not require RHIG. They would receive an unnecessary blood product exposure. • 14.2% of individuals (unclassified, DAR) would be classified as Rh POS. Current evidence suggests that with-holding RHIG in such cases may result in RhD alloimmunization but whether this translates into a risk for HDFN is uncertain. • How to decrease the number of NOT AT RISK individuals (WDT 1,2,3,4,) classified as Rh NEG while correctly identifying individuals AT RISK for RHD alloimmunization?
Enhancement Techniques • Extended incubation: 5’ incubation added to tube testing with S4 and S5 to standardize technique - 10/12 samples reclassified to Rh POS but 3/10 shown to have ‘weak expression of D, unclassified’ on molecular analysis. • Conclusion: Extended incubation may assist in minimizing the number of individuals typed inappropriately as Rh NEG. However, some of the individuals whose Rh type changed from NEG to POS may be at risk for D alloimmunization.
Reanalyzed Data to Determine Implications of Adding Novaclone to Algorithm (Novaclone ≥ 2+ = Rh POS) • 59% (57/97) of NOT AT RISK patients would continue to have RHIG recommended unnecessarily (versus 97% without Novaclone) – mainly WDT1 and 2 • 19% (10/53) (9 ‘unclassified’ & 1 DAR) AT RISK patients would be designated Rh NEG & RHIG recommended appropriately • 81% (43/53) (42 ‘unclassified’ & 1 DAR) would be designated Rh POS & ineligible for RHIG. DAR is known to be at risk for anti-D formation; whether the ‘unclassified’ cases are at risk is uncertain.
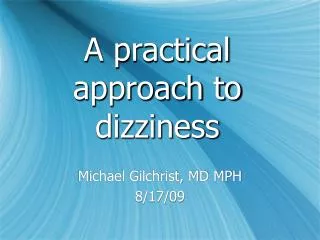
CBS Edmonton Rh Discrepancy Algorithm for Prenatal Testing *Tube Test – Direct Agglutination (DA) is 5 min RT incubation for S4 & S5. **Rh Discrepancy with previous testing – review historical results to ensure there isn’t a collection error. Comment 1 – This patient appears to have a weak expression of the D antigen and may be capable of forming Anti-D. Patient could be reported as RhD positive by another laboratory that uses different RhD antisera. Comment 2 – Rh Immune Globulin to be give at discretion of physician. Comment 3 – Patient may have been previously reported as Rh negative. This patient probably has a weak or variant D antigen and may be capable of forming anti-D. Comment 4 – Unable to determine Rh typing at this time. Current testing shows variable results with different anti-D typing sera. Until Rh(D) type is determined consider patient as Rh(D) negative and eligible for antenatal Rh Immune Globulin. Comment 5 – Sample has been forwarded for RHD genotyping to______________________ .
Further Investigation of Unclassified Cases Initial Testing:RhD multiplex PCR for exons 3-7 PCR-RFLP for weak D types 1, 2, 3, 4 Direct sequencing of exons 5 and 7 28 unresolved samples further investigated using a Qiagen DNA extraction kit (Hilden, Germany) and BAGene DNA-SSP Partial D-Type kit (Lich, Germany). This kit is able to identify D categories II, III, IV, V, VI, VII as well as partial D DAU, DBT, DFR, DHMi, DHMii, DNB, DHAR and DEL. Results:Allelic assignment was resolved in 16/28 (57%) samples.13 D category VII 2 DHMi 1 D category IIIa/c/IV (further testing b/c phenotype not concordant with DNA findings) 12 Unresolved (pattern consistent with standard D allele) Reference: Pavenski K, Denomme G, Hannaford K, Appados A, Hannon J. Identification of Partial D Variants in Prenatal Specimens with Serologically Weak or Undetermined D. Transfusion 2008; 48 (Suppl): 185A
Current Developments • Molecular testing not widely available in Canada and expensive approach to resolving RhD discrepancies. • Slight variations in algorithms in use in CBS Perinatal Laboratories. • CBS Perinatal Committee is working towards a standardized algorithm which is agreeable to all provincial prenatal laboratories and which will facilitate implementation of the new CBS LIS system in June 2010. • Efforts are aimed at improving the algorithm for identification of AT RISK patients and minimizing unnecessary RHIG administration to NOT AT RISK patients. • Novaclone and/or enhancement techniques such as extended incubation (or both) being considered. • An effort is being made to ensure that physicians & hospitals are aware of RhD discrepant results detected in CBS prenatal laboratories, through the use of coded comments & the inclusion of Novaclone results on patient reports. • CBS is liaising with hospitals to minimize the number of discrepant RhD typing results and the impact for patient care.
CBS Perinatal Committee • Kathy O’Shea, BC & Y • Gerri Growe, BC & Y • Judith Hannon, AB (Chair) • Jean Ashdown, AB • Debra Lane, MB • Lee Grabner, MB • Robert Fallis, MN • Ted Alport, SK • Greg Denomme, Toronto • Janet Barnes, NRL • Gwen Clarke, AB • Gerri Barr, AB • Vivian Stephens, BC & Y • Judy Boland, MB • Lynn Meilleur, MB • Tony Dolnik, BC & Y • Bernie Eurich, SK • Satinder Walia, Toronto • Heather Hume, Head Office
“Variable” D results CBS perinatal results differ from hospital results Previously positive; new reagent or method, now negative Previously negative; new reagent or method, now positive Doctors confused Lab credibility suffers a blow
Variable D results A particular combination of results does not always predict what the “molecular” or genetic D type really is Shall we call them all Rh negative?
Is all variability = Rh negative in a recipient? Rh negative blood is a scarce resource Not all weak or partial D individuals are at risk for allo immunization – in fact – most are not! RhIg is a human blood product… should we always err on the side of administering RhIg?
Additional controversy • Should 1+ be considered positive or negative? • And the reaction strength is method specific • Should front line staff be expected to record or enter clear positive results as negative? • Will the LIS allow blood group interpretation if weak reactions are present and the interpretation doesn’t match? • What if a genotyping report is available?
Lab considerations What is the discrepancy due to Don’t forget mis- collection or misidentification as a cause for discrepancy How do you report weak or variable reactions How do you resolve discrepancies between testing episodes or between labs
Clinical Considerations The risk of developing an anti D The risk of RhIg The risk of HDN
Mom and cord testing A pregnant woman is a potential recipient of fetal red cells and may be immunized if she is weak or partial D positive; Categorize as Rh negative if weak or discrepant reactions A neonate is a potential blood donor (to mom) and may immunize mom if weak or partial D positive Categorize as Rh Positive for purposes of maternal RhIg eligibility IAT (weak D testing) required for all Rh Negative neonates/cord samples
Neonatal transfusion recipients Neonate/cord sample may be Rh positive for maternal RhIg eligibility and Rh negative for pre transfusion testing Cord samples should not be treated as pre transfusion samples
What’s a transfusion lab to do?! Know your reagent – is it limited specificity and likely to pick up partial D… or is it broad specificity and likely to make all weak and partial D Rh Pos? Avoid weak D (IAT) testing as a routine test in D negative individuals Consider using the same method/reagent as nearby labs or sites that provide reference testing
Continued…. Determine the strength of reactivity that you consider positive (is 1+ positive?) Standardize a method to be your “gold standard” and use these results to guide your results – but acknowledge the variability in your report Consider reference lab RHD genotyping to resolve weakly reactive D and or discrepant results
Donor Retesting and Cord samples Use broad specificity anti D reagents (a monoclonal polyclonal IgM/IgG blend) Weak D testing must be done on Rh negative or discrepant samples Cord weak D test results should be used for determination of maternal RhIg eligibility and not for pre transfusion testing
Reporting Results discrepant from historical or blood donor records should be explained (admit defeat in your report) RHD genotyping (if done) should become a part of the permanent record for that individual –along with an explanatory comment Cord and neonatal typing discrepancies also require explanation
Example report: Rh(D) typing is variable with different methods and reagents. This usually indicates a weak or partial D antigen. RhIg administration is at the discretion of the patient and attending physician
Patient scenarios 37 year old G4P3; has never received RhIg previously (always typed as Rh pos). Now types with your new reagent/analyzer as 1+ and negative. Has no detectable anti D. Plans no further children with tubal ligation to follow delivery… recommendation?
Patient 2 • 24 year old G2P2 with discrepant D result identified on postnatal sample for RhIg eligibility (now is Rh positive; previously typed as Rh negative) has previously received RhIg… recommendation?
The End Questions?