Download
1 / 15
160 likes | 423 Views
ANTINEOPLASTIC AGENTS. PATHOLOGY PHARMACOLOGY. LECTURE 9. Neoplasia. New growth

E N D
ANTINEOPLASTIC AGENTS PATHOLOGY PHARMACOLOGY LECTURE 9
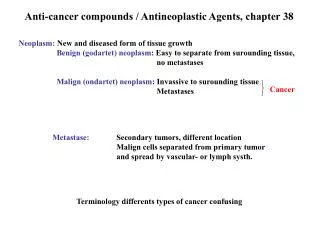
Neoplasia • New growth • Abnormal mass of tissue the growth of which exceeds and is uncoordinated in comparison to that of the normal tissue and continues even in the absence of the stimulus that initiated the growth of the tissue in this manner. • Clinically divided into benign and malignant types
Malignant Neoplasia Benign Neoplasia Common terms-cancer or crab-due to their strong adherence properties Can affect neighboring and far away tissues (metastasis) Large, poor demarcation, faster growth, invasive Drug treatment plus surgery No specific nomenclature: Suffix –sarcoma/ carcinoma for mesenchymal tissue like fibrosarcoma, squamous cell carcinoma, adenocarcinoma, HCC, etc Leukemia, lymphoma, etc • Innocent • Localized • Small, demarcated, well differentiated • Surgical removal • Can progress to malignancy • Nomenclature:suffix–oma • Examples: Fibroma, lipoma, osteoma, meningioma, papilloma (glands), hepatoma, etc
Clinical Characteristics- To decide the candidature of cancer chemotherapy 1. Differentiation and Anaplasia- Benign tumors are well differentiated to perform the normal functions of the tissue. Malignancies are anaplastic (anaplasia-dedifferentiated) and pleomorphic. (Not to be confused with dysplasia – abnormal but non-malignant malfunctioning)
2. Rate of growth Low risk: Low grade, well differentiated tumour, Gleason score 2–6Intermediate risk: Intermediate grade, moderately differentiated, Gleason score 7High risk: High grade, poorly differentiated, Gleason score 8–10 3-10
ETIOLOGY • Geographical – sun, UV, oxygen deficiency • Environmental – asbestos, benzene, phenol • Age – breast, prostrate • Hereditary – protooncogenes, tumour suppressor genes, DNA repair • Acquired – hyperplastic, dysplastic, gastritis induced, leukoplakia (betel leaf)
Oncogenes CURRENT TARGETS Cell cycle Apoptosis Tumor Suppressor Inv. and Mets Angiogenesis
PHARMACOLOGY OF ANTINEOPLASTIC AGENTS NEXT LECTURE