Download
1 / 21
210 likes | 368 Views
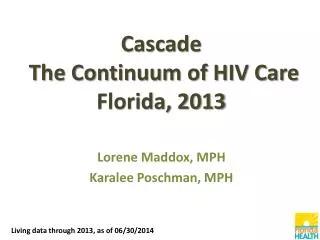
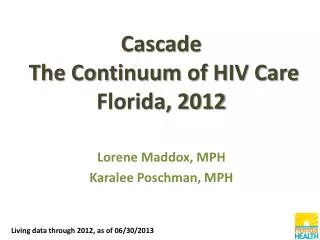
IMPLEMENTING CLINICAL RECOMMENDATIONS: ART STRATEGIES, TOOLS, AND HEALTHY SYSTEMS/SERVICE DELIVERY RECOMMENDATIONS 11-14: ADHERENCE John G. Bartlett Johns Hopkins University School of Medicine . The Continuum of HIV Care -- US. 80%. 77%. 66%. 89%. 77%.

E N D
IMPLEMENTING CLINICAL RECOMMENDATIONS: ART STRATEGIES, TOOLS, AND HEALTHY SYSTEMS/SERVICE DELIVERYRECOMMENDATIONS 11-14: ADHERENCEJohn G. BartlettJohns Hopkins UniversitySchool of Medicine
The Continuum of HIV Care -- US 80% 77% 66% 89% 77% Of all with HIV infection, 850,000 individuals do not have suppressed HIV RNA (72%) MMWR (60), 2011
ART Strategies • Among regimens of similar efficacy and tolerability, once-daily regimens are recommended for treatment-naivepatients beginning ART (II B). • Switching treatment-experienced patients receiving complex or poorly tolerated regimens to once-daily regimens is recommended, given regimens with equivalent efficacy (III B). • Among regimens of equal efficacy and safety, fixed-dose combinations are recommended to decrease pill burden (III B).
Adherence Tools for Patients • Reminder devices and use of communication technologies with an interactive component are recommended (I B). • Education and counseling using specific adherence-related tools is recommended (I A).
Education and Counseling Interventions • Individual one-on-one ART education is recommended (II A). • Providing one-on-one adherence support to patients through 1 or more adherence counseling approaches is recommended (II A). • Group education and group counselingare recommended; however, the type of group format, content, and implementation cannot be specified on the basis of the currently available evidence (II C). • Multidisciplinary education and counselingintervention approaches are recommended (III B). • Offering peer support may be considered (III C).
THE NON-VALUE OF PILL COUNTS: FEM-PrEP (Van Damme. NEJM 2012) Trial: Randomized, double-blind placebo-controlled trial in 2,120 HIV negative women in South Africa. Results Placebo TDF/FTC n=1,058 n=1,062 Adherence report 95% 95% Pill counts 88% 88% TDF levels >10 ng/mL Failure ----- 15% No failure ----- 24%
WHAT TO START Guideline Backbone 3rd Drug DHHS, IAS-USA TDF/FTC EFV, RAL, British ATV/r, DRV/r European TDF/FTC EFV, NVP ABC/3TC ATF/r DRV/r LPV/r, RAL WHO TDF/3TC EFV, NVP AZT/3TC
ART REGIMEN: REGIMEN SELECTION Goal: NDV, avoid resistance, ADR Factors in the decision: • Baseline resistance test • Co-morbidities: Core, Renal, HBC, Pregnancy, Psychological issues • Potency: Undefeated regimens • Urgency: Pregnancy, HIVAN, AIDS, Primary HIV • Resistance to resistance: FOTO (EFV) and PI/r • Cost and coverage
WHAT TO START: PILL BURDEN Regimen x/d Pills EFV/TDF/FTC* 1 1 ATV/r/2 NRTIs 1 3 DRV/r/2 NRTIs 1 4 RAL/2 NRTIs 2 3 *RPV/TDF/FTC
Study 236-102: ATRIPLA VS. QUAD IN TREATMENT-NAÏVE (N=700): HIV-1 RNA < 50 copies/mL(Sax P. 2012 CROI. Abstr. 101) +3.6%, 95% CI 3.6 (-1.6% to +8.8%) CD4+ change: Quad +239vs. EFV +206 c/mm3 (p=0.009) Sax P, et al. 19th CROI; Seattle, WA; March 5-8, 2012. Abst. 101.
COST OF CARE Contemporary costs/yr. (AIDS 2010;24:2705) • HAART $12,000 (72%) • Meds (other) $ 2,100 • In-patient $ 600 • Out-patient $ 400 Total (Meds) $ 16,600 Growth: 40,000/yr survival + T&T all: $800 million
US Patent Expirations AZT/3TC NVP GS7340 = 2025 AZT/3TC/ABC ABC/3TC TDF/FTC VVC* (SP) RAL 2022-5 EFV MVC ETR DLV ddC ddI TDF d4T 3TC ABC AZT EVG RPV 09 05 07 19 20 21 22 23 06 08 10 11 12 13 14 15 16 17 18 ATV NFV LPV/ RTV caps LPV/RTV tabs RTV IDV SQV CVC= 2023+ TPV DRV RTV boosting 12
Dhhs guidelines 2012 VL CD4 Pre ART 3-6 mos. 3-6 mos. Start Baseline Baseline 2-8 wks* ----------- On ART 3-6 mos. 3-12 mos. *week VL (log 10 c/mL 1 -0.75-1 4 1.5-2 8-16 <500 24-48 <50
P4P4P: THE STATUS OF PAYING PATIENTS FOR SELF CARE Practice: Widespread and international Incentives: Cash, groceries, lottery tickets, meal tickets. Conditions: Chronic – smoking, obesity , BP control, diabetes, HIV HIV trial: HPTN 65 – Controlled trial, (unblinded) HIV test – $25, Enroll in care – $70, NDV – $280/yr (1.7% of HIV care cost) Status: Widely practiced, no one wants to talk about it.
A TEST OF FINANCIAL INCENTIVES TO IMPROVE WARFARIN ADHERENCE(Volpp KG. BMC Health Sys Res 2008;8:272)
THE POWER OF HOPE (Harris J, De Angelis. JAMA 2012;300:2912) “With a deeper understanding of the science of care, physicians will increasingly realize that a meaningful patient-physician relationship leaves each patient better able to adhere to the treatment plan.”
HEALTHCARE OUTCOMES IN HIV:REDUCING DISPARITIES (Moore R. CID; in press) Issue: Major issue in HIV care is retention in care and adherence Method: Moore Clinic data 1995-2010 N=6,366 Pt/yrs 27,941 Demographics: B – 77%, F – 34% Risk: IDU-45%; MSM – 30% Insurance: Private – 15% Results: Calculated life expectancy at age 28 yrs = 73.4 yrs for all groups – race, gender and risk
HEALTHCARE OUTCOMES IN HIV:REDUCING DISPARITIES (Moore R. CID; in press) Issue: Major issue in HIV care is retention in care and adherence Method: Moore Clinic data 1995-2010 N=6,366 Pt/yrs 27,941 Demographics: B – 77%, F – 34% Risk: IDU-45%; MSM – 30% Insurance: Private – 15% Results: Calculated life expectancy at age 28 yrs = 73.4 yrs for all groups – race, gender and risk
VL FOR 3 HIV RISK CATEGORIES OVER TIME(Moore RD. CID 2012; in press)
ART ADHERENCE IAPAC GUIDANCE: Scientifically validated systematic approaches Regimen selection: • Drugs that will work (science) • Drugs patients will take (art) Factors to consider: • Documentation metric: VL • Impact of patent expiration • Cost-support services • P4P4P • Clinic viral load