Download
1 / 42
430 likes | 594 Views
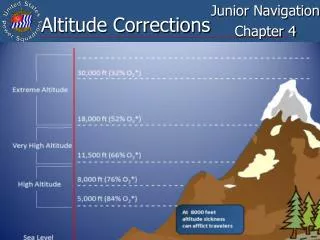
Acute Effects of Altitude. Rapid Ascent (Loss of Cabin Pressure): Hypoxia Sleepiness, laziness False sense of well-being Impaired judgment Blunted pain perception Increasing errors on simple tasks Decreased visual acuity Clumsiness Tremors Loss of consciousness or even death.

E N D
Acute Effects of Altitude Rapid Ascent (Loss of Cabin Pressure): Hypoxia Sleepiness, laziness False sense of well-being Impaired judgment Blunted pain perception Increasing errors on simple tasks Decreased visual acuity Clumsiness TremorsLoss of consciousness or even death
Acute Effects of Altitude Ascent to Moderate Altitude (Acute Mountain Sickness): Hypoxia and Hypocapnia; Alkalosis Headache, Dizziness Breathlessness at rest Weakness Malaise Nausea, anorexia Sweating, palpitations Dimness of vision, partial deafness Sleeplessness Fluid retention Dyspnea on exertion
ALVEOLAR AIR EQUATION PACO2 PAO2 = PIO2 - + F R PACO2 PAO2 = FIO2 2 R ( PB - PH O) -
. . HPV HELPS MAINTAIN V / Q O2 = 100 torr CO2 = 40 torr Decreased O2 Increased CO2
Pco2 , pH temp, BPG 100 80 Pco2 , pH temp, BPG 60 Hemoglobin saturation, % 50% 40 20 20 40 60 80 100 120 140 160 P50 Partial pressure of oxygen, torr
Physiologic Responses to High Altitude Relative to Sea Level Control Values IMMEDIATE EARLY ADAPTIVE (72H) LATE ADAPTIVE (2 to 6 WEEKS) Spontaneous Ventilation Minute ventilation Respiratory rate Tidal volume Arterial Po2 Arterial Pco2 Arterial pH Arterial HCO3- Evaluation of Lung Function Vital capacity Maximum airflow rates Functional residual capacity Ventilatory response to inhaled CO2 Ventilatory response to hypoxia Pulmonary vascular resistance Variable , Variable , Variable ,
Physiologic Responses to High Altitude Relative to Sea Level Control Values IMMEDIATE EARLY ADAPTIVE (72H) LATE ADAPTIVE (2 to 6 WEEKS) Oxygen Transport Hemoglobin Erythropoietin P50 2,3 - BPG Cardiac output Central Nervous System Headaches, nausea, insomnia Perception, judgment Spinal fluid pH Spinal fluid HCO3 Cerebral edema , -
Arterial Blood Gases and Oxygen Content in Climbers on Mount EverestGrocott, et al., NEJM 360:140-149, 2009 Samples taken at 8440 m (=27,559 ft) From 4 climbers who had reached summit Breathed ambient air for 20 minutes Barometric pressure = 272 mm Hg
Arterial Blood Gases and Oxygen Content in Climbers on Mount Everest (n = 4)Grocott, et al., NEJM 360:140-149, 2009 P barom =272 mm Hg PAO2 = 30.0 mm Hg PaO2 = 24.6 mm Hg SaO2 =54% [Hb] = 19.3 g/100 ml blood CaO2 = 14.58 ml O2/100 ml blood pHa = 7.53 PaCO2 = 13.3 mm Hg [HCO3-] = 10.8 mmol/liter
Diving PhysiologyPhysiologic Stresses The severity of the stress depends on the depth attained, the length of the dive, whether the breath is held, or breathing apparatus is used. Major physiologic stresses: • Elevated ambient pressure • Decreased effect of gravity • Altered respiration • Hypothermia • Sensory impairment
air seawater
Breath-hold Diving Submarine Scuba Diving air seawater 99 feet 1 atm 4 atm 4 atm
Effects of immersion up to the neck Respiration : Pressure outside chest wall is now positive, averaging about 20 cm H2O. Intrathoracic pressure is less negative at end-expiration. • FRC decreases about 50% • ERV decreases about 70% • VC – slight decrease • IRV increases • Slight decrease in RV, probably due to increased pulmonary blood volume Result: about 60% increase in the work of breathing
Effects of immersion up to the neck Cardiovascular : • Increased venous return due to elevated abdominal pressure and decreased pooling in peripheral veins. (decreased ambient temperature will also lead to venoconstriction). • Increased venous return leads to increased central blood volume (approximately 500 ml). Right atrial pressure increases from about –2 to +16 mmHg. • Cardiac output and stroke volume increase about 30%. • Ventilation perfusion probably better matched.
Effects of immersion up to the neck Renal : • Elevated intrathoracic blood volume “immersion diuresis”. Urine flow increases 4-5 times but osmolal clearance increases very slightly. • Consistent with ADH suppresion or release of atrial natriuretic hormone.
The Diving Reflex • Vagally mediated bradycardia • Sympathetically mediated increased systemic vascular resistance, contraction of spleen • Same effect as chemoreceptor stimulation without lung inflation reflex • Sensors unknown in man
100 Partial Pressure (mmHg) 0 0 20 40 60 Time (sec) Rest Work O2 CO2
Dive 1 Atm Partial Pressure (mmHg) O2 100 CO2 0 Descent 2 Atm 0 20 40 60 Time (sec)
Gas exchange during a 10 meter, one minute breath-hold dive • Usually hyperventilate first • Compression during descent, expansion during ascent Before: After: PAO2 = 41mmHg PACO2 = 42mmHg PAN2 = 631mmHg Surface: PAO2 = 120mmHg PACO2 = 29mmHg PAN2 = 567mmHg 10 meters depth : PAO2 = 149mmHg PACO2 = 42mmHg PAN2 = 1143mmHg
Therefore, the transfer of O2 from alveolus to blood is undisturbed until ascent. However, the normal transfer of CO2 from blood to alveolus is reversed during descent and results in a significant retention of CO2 in the blood.
Physiologic Problems Encountered in Diving With Underwater Breathing Apparatus Increased work of breathing – not as great a problem since breathing gases at ambient pressure. However, increased gas density leads to increased airway resistance work of breathing. Helium is 1/7 as dense as N2, so at great depths breathe He-O2 mixture. Respiratory sensitivity to CO2 is decreased at depth because of low breathing rates, high Po2 and increased gas density
Other Hazards at Depth • Barotrauma • Descent (squeeze): • Ears • Sinus • Dental • Pulmonary – congestion, edema, hemorrhage • Ascent: • Ear • Sinus • Dental • Pulmonary – “Burst Lung” – pneumothorax, air embolism • GI – eructation, flatus, abdominal discomfort
Decompression IllnessArterial Gas Embolism and Decompression Sickness • During diving the high ambient pressure PN2. The high PN2 helps dissolve this normally poorly soluble gas in the body tissues, especially fat, which has a relatively high N2 solubility. Therefore, tissues become supersaturated with N2 • During rapid ascent, the high ambient pressure falls rapidly, and bubbles of N2 form in the blood and body tissues, especially the joints and more dangerously, the CNS. • Treatment : Recompression chamber • Prevention : Decompression tables : He instead of N2 (He is about ½ as soluble as N2) • Can also get if travel in an airplane to soon after a dive
Nitrogen Narcosis – high PN2 directly affects CNS – at 100 ft.: euphoria, loss of memory, irrational behavior, etc. At greater depths : numbness of limbs, disorientation, motor impairment, loss of consciousness. Mechanism of N2 narcosis is unknown. • Oxygen Toxicity – inhalation of 100% O2 at 760 mmHg or lower [O2] at higher pressure can cause both alveolar and CNS damage (convulsions at greater than 2.5Atm.) Mechanism of O2 toxicity is not known. • High Pressure Nervous Syndrome – at very great depths divers experience decreased manual dexterity and tremors. Can be prevented by adding very small amounts of N2 to the inspired gas mixture.