Download
1 / 7
70 likes | 76 Views
The article Liver Transplant in India involves data with respect to Liver working, indications of liver disappointment, liver gift, and Liver medical procedure. Expectation this article can convey mindfulness with respect to liver transplant to all peruses.

E N D
Liver Transplant in India Liver is a vital part for humans; it plays a crucial role in metabolism process. If the liver is damaged by any means the victim cannot survive. The best option for him/her would be Liver Transplant. The article Liver Transplant in India comprises of information regarding liver functioning, signs of liver failure, liver donation, Liver surgery. Hope this article can bring awareness regarding liver transplant to all readers. LIVER FUNCTION The liver is a vital organ, which means that you cannot live without it. The liver performs many critical functions, including the metabolism of toxins and drugs, the elimination of degradation products of normal metabolism (eg, the removal of bilirubin and ammonia from blood), and the synthesis of many enzymes and proteins (blood coagulation factors). Blood enters the liver from two channels, the portal vein and hepatic artery, providing nutrients and oxygen to liver cells, also known as hepatocytes, and other name is bile ducts. The blood leaves the liver through the hepatic veins that flow into the inferior vena cava that immediately enters the heart. The liver produces bile, a liquid that helps to eliminate metabolic waste and toxins through intestine and dissolve fats. Each hepatocyte creates bile and excretes it into microscopic channels that join to form bile ducts. Like tributaries that join to form a river, the bile ducts join together to form a single “hepatic duct” that brings bile into the intestine. WHO NEEDS A LIVER TRANSPLANT? Liver transplantation surgically replaces a diseased or failing liver with a healthy, normal liver. Currently, transplantation is the only cure for liver failure because no machine reliably provides all the functions of the liver. People who need a liver transplant usually have one of the following conditions. ACUTE HEPATIC INSUFFICIENCY Acute liver failure, also known as fulminant hepatic failure, occurs when a previously healthy liver is massively injured with clinical signs and symptoms of liver failure. A number of things can lead to acute liver failure, but the most common causes are ingestion of a toxin such as fungi poisonous or an idiosyncratic reaction, overdose of acetaminophen, viral infections. The characteristic of this condition is the development of confusion (encephalopathy) within eight weeks after the onset of yellowing of the skin (jaundice). The confusion occurs because the toxins
usually metabolized by the liver accumulate. Patients with acute liver failure can die within days if not transplanted. These patients are classified as absolute priority (status I), which places them at the top of the waiting lists for the liver of a donor. CHRONIC HEPATIC INSUFFICIENCY The liver has a remarkable ability to repair itself in response to an injury. Nevertheless, repeated lesions and repairs, usually over many years and even decades, heal the liver permanently. The final stage of healing is called cirrhosis and corresponds to the point where the liver can no longer repair itself. Once a person has cirrhosis, they may begin to show signs of liver failure. This is called decompensated liver disease. Although medications can reduce symptoms caused by liver failure, liver transplantation is the only permanent cure. SIGNS OF LIVER DAMAGE Gastrointestinal bleeding: As the liver becomes more resistance, scarred to portal blood flow increases, resulting in increased pressure in the portal venous system. This portal hypertension requires alternative ways for the blood to return to the heart. The small veins in the abdomen, but outside the liver, then become enlarged and thin-walled because of the abnormally high amount of blood that passes through them under increased pressure. These fragile veins, called varicose veins, often line parts of the gastrointestinal tract, especially the stomach and esophagus, and are likely to rupture and bleed. When bleeding takes place in the intestinal tract, it can be fatal. FLUID RETENTION A function of the liver is to synthesize many of the circulating proteins in the blood, including albumin. Albumin and other proteins in the blood stream retain fluid in the vascular space by exerting what is known as oncotic (or osmotic) pressure. In case of hepatic insufficiency, the low albumin levels cause the liquid to come out of the blood which cannot be reabsorbed. The fluid accumulates in the body cavities and tissues, most often in the abdominal cavity, called “ascites”. The fluid can also accumulate in the thoracic cavity or in the legs. Fluid retention is treated first of all by a strict limitation of the dietary salt supply, then by drugs (diuretics) which force the loss of salt and water by the kidneys and finally by intermittent drainage by insertion of a needle in the abdominal or thoracic cavity. ENCEPHALOPATHY
The inability of the liver to remove ammonia and other toxins from the blood allows these substances to accumulate. These toxins cause cognitive dysfunction that ranges from sleep-wake cycle disorders to mild coma confusion. JAUNDICE One of the main functions of the liver is to eliminate the breakdown products of hemoglobin. Bilirubin is one of those degradation products treated and excreted by the liver. In cases of hepatic failure, bilirubin is not eliminated from the body and bilirubin levels increase in the blood. The skin and all the tissues of the body then take on a yellow color. CAUSES OF CHRONIC LIVER INJURY VIRAL HEPATITIS HEPATITIS B Around 5% of all liver transplants in India happens because of hepatitis B but represents a higher proportion of liver transplants in other parts of the world, including Australia / New Zealand. HEPATITIS C Most of the liver transplants in India happens because of hepatitis C, affecting nearly 50% of all liver transplant recipients. ALCOHOLIC LIVER DISEASE Hepatic impairment due to alcohol abuse is the second most common indication of liver transplantation in India. Most centers require a minimum of six months of abstinence, often as part of a recognized addiction treatment program such as Alcoholics Anonymous, as a condition of registration for transplantation. METABOLIC LIVER DISEASE Nonalcoholic Steatohepatitis (NASH): Deposition of fat in liver cells can lead to inflammation that injures and heals the liver. Risk factors for the development of fatty liver and NASH include obesity and metabolic conditions such as diabetes and hyperlipidemia (increased cholesterol). The percentage of patients transplanted for this disease has increased 35-fold between 2000 and 2005.
HEPATOCELLULAR CARCINOMA Hepatocellular carcinoma (HCC) is a primary liver cancer, which means that it comes from abnormal liver cells. CHC rarely occurs in a normal, non-cirrhotic liver. Its incidence is, however, remarkably increased in the context of cirrhosis and, in particular, certain types of liver diseases leading to cirrhosis. Although cancer begins in the liver first, as it grows, it can spread to other organs of the victim, a process called metastasis. Hepatocellular carcinoma is most commonly spread to the bones or lungs. The risk of spreading out of the liver increases with the size of the cancer. Liver transplantation definitely cures a patient with HCC, provided that the tumor has not spread beyond the liver. Because there are many more people in need of liver transplants than organs available, so specific guidelines called the Milan Criteria have been established to define which HCC patients can be transplanted. These criteria define the limits of the number and size of tumors that ensure a very low probability of cancer spreading outside the liver. WHO ARE NOT CANDIDATES FOR A LIVER TRANSPLANT There are many people with decompensate liver disease and cirrhosis, but not all are suitable candidates for liver transplantation. A patient should be in a position to survive the operation and also potential postoperative complications, reliably take drugs that prevent infections, travel to the clinic regularly, and undergo laboratory tests and stop drinking alcohol. The conditions listed below are generally considered absolute contraindications to liver transplantation. Life expectancy may be reduced due to Serious and irreversible illness Severe pulmonary hypertension Cancer that has spread to other organs outside the liver Uncontrollable or Systemic infection Abuse of active substances (alcohol and / or drugs) Unacceptable risk of substance abuse (alcohol and / or drugs) History of incompletion or adoption to a strict medical course. Uncontrolled and Severe psychiatric illness TYPES OF ORGAN DONORS
BRAIN DEAD DONOR ORGANS Most livers used for transplantation come from dead brain patients. Brain death is usually due to a major stroke or massive head trauma caused by a penetrating injury (eg example a gunshot wound) or a blunt injury (for example, accidents). The trauma has stopped all brain functions, although other organs, including the liver, can continue to function normally. There are strict definitions as to what constitutes brain death based on the complete absence of any kind of brain function. Because patients who meet the criteria for brain death are legally dead, they are appropriate tissue and organ donors. In countries like United States, the family of someone who is brain dead must give consent for organ and / or tissue donation and in France, consent to organ donation is presumed and allowed, but the family members have right for objection. Typically, transplant centers whose patients will receive organs from a particular donor will send a team of surgeons to procure the appropriate organ. The organ harvesting procedure takes place in an operating room of the donor hospital. The organs are removed and stored in order to optimize their state during the period of storage and transport. Each acquired organ is then transported to the hospitals where the designated recipient is waiting for it. ORGAN DONORS OF CARDIAC DEATH Sometimes a patient has a poor neurological prognosis and a devastating brain injury, but does not meet the strict criteria for brain death in that there is still detectable brain function. In these situation, the patient’s family may decide to withdraw lifesaving medical support and allow him to die. In such type of cases, death is treated as cardiac death but not as brain death. Organ donation can happen after cardiac death but make sure family members must accept it. It is only after the family’s decision to withdraw support that the patient can be considered for an organ donation after his death. In this senario, support is withdrawn, according to the wish of family members and managed by the patient’s physician, and then the patient is allowed to die. The patient’s physician, who is not involved in any aspect of the organ transplant, is present to determine when the heart stops beating and the circulation is stopped so that the patient has no sign of life . He or she then declares the patient’s death. An urgent operation is then performed to preserve and remove organs for transplantation. This mode of cardiac death, unlike brain death, causes an increase in organ damage during two periods. The first
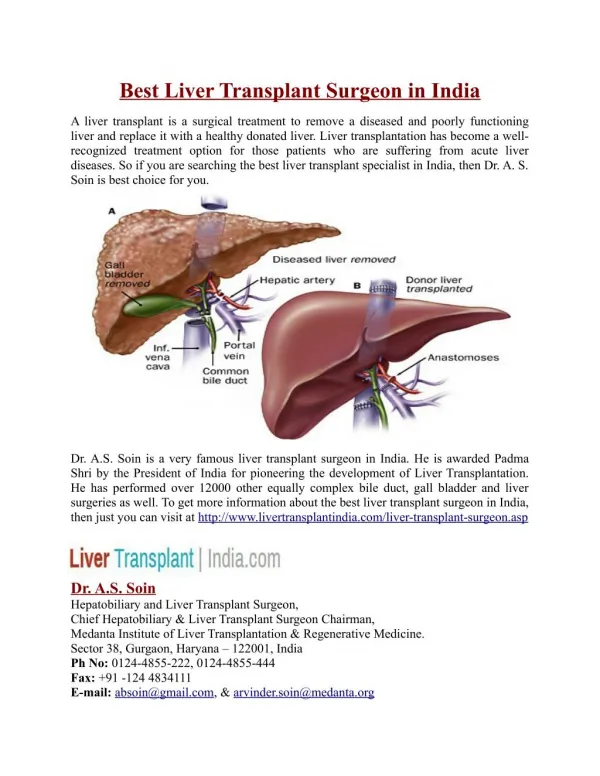
period is that between the withdrawal of support from life and death. As the donor’s breathing and circulation deteriorate, the organs may no longer receive enough oxygen. The second period is minutes immediately after death and until the organs are rinsed with the preservative solution and cooled. As a result, livers obtained from cardiac death donors are associated with an increased risk of primary malfunction or dysfunction of the early organs, thrombosis of the hepatic arteries and biliary complications. LIVING DONORS Although each person has only one liver and would die without it, it is possible to donate part of the liver for transplantation to another individual. Segmental anatomy (see figure below) allows surgeons to create grafts of varying size, depending on the recipient’s requirement for liver tissue. Partial livers in the recipient and donor will develop to provide normal liver function for both individuals. THE LIVER TRANSPLANT OPERATION A liver transplant involves the removal and preparation of the donor’s liver, the removal of the diseased liver, and the implantation of the new organ. The liver has several important connections that must be re-established so that the new organ can receive blood flow and drain the bile from the liver. The structures to be reconnected are the the bile duct, the hepatic artery, the portal vein and inferior vena cava. The exact method of connecting these structures varies depending on the specific anatomy of the recipient and the anatomy of donor and, in some cases, the recipient’s disease. For a person undergoing liver transplant surgery, the series of events in the operating room is as follows: Incision Evaluation of the abdomen for abnormalities that would prevent liver transplantation (eg, undiagnosed infection or malignancy) The native liver is mobilized.(dissection of hepatic attachments to the abdominal cavity) Isolation of important structures (hepatic artery, common bile duct, portal vein, behind and below the liver, inferior vena cava above) Transaction of the structures mentioned and removal of the native sick liver. Sewing in the new liver: First, venous blood flow is restored by connecting the inferior vena cava and the portal veins of the donor and recipient. Then, the arterial flow is restored by sewing the recipient and
donor hepatic arteries. Finally, biliary drainage is done by sewing the common bile ducts of the recipient and donor. Bleeding need to be controlled The incision is closed.