Download
1 / 45
460 likes | 671 Views
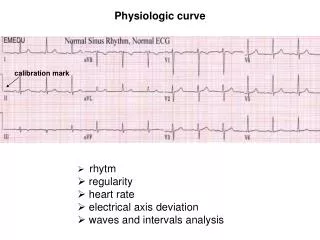
Physiologic curve. calibration mark. rhytm regularity heart rate electrical axis deviation waves and intervals analysis. Rhytm. Sinus rhytm 60 – 90 / min Junctional (Nodal) 40 – 60 / min Idioventricular 30 – 40 / min Atrial fibrilation Atrial flutter.

E N D
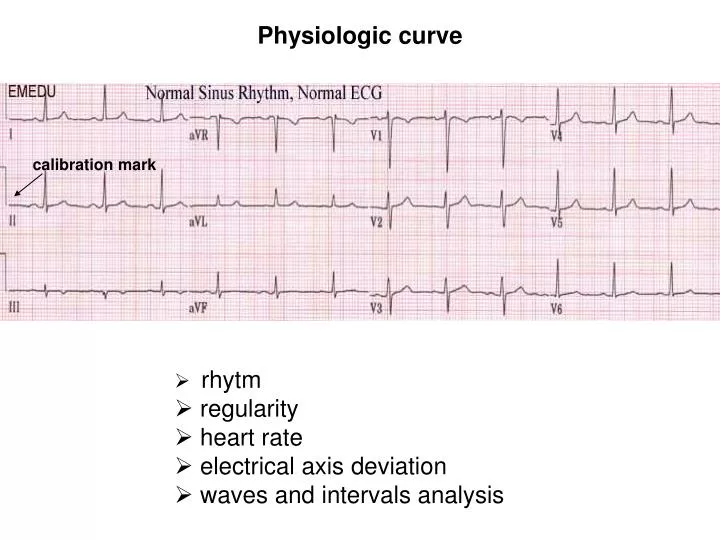
Physiologic curve calibration mark • rhytm • regularity • heart rate • electrical axis deviation • waves and intervals analysis
Rhytm Sinus rhytm 60 – 90 / min Junctional (Nodal) 40 – 60 / min Idioventricular 30 – 40 / min Atrial fibrilation Atrial flutter the most frequent rhytm pathologies
Regularity Regular – the R-R intervals are constant Irregular – variable R-R intervals – respiratory sinus arrhytmia The most frequent pathologies: atrial fibrilation extrasystolas Heart rate Normal range 60 – 90 Tachycardia 90 Bradycardia 60
normal -30° - +105° right axis deviation left axis deviation Heart axis - is an average of all depolarizations in the heart - direction of depolarization (vector) of the QRS complex - the left ventricle is thicker so the mean QRS vector is down and to the left - the QRS axis may shift due to physical change in the position of the heart, chamber hypertrophy, or conduction block
Spikes and waves analysis wave P - 2,5 mm, 0,1 s - aVR always, leads III and V1 sometime negative - sinus rythm, II negat → junction P pulmonale– tall, narrow, peaked above 2,5 mm P mitrale – broad, bifid
Spikes and waves analysis PQ interval – isoelectric, 0,12-0,2 s – changes with the hear rate prolongation up to 0,2 s - AV block of 1st degree QRS complex– depolarization of ventricles voltage criteria (hypertophy x obesity, exsudate) abnormál shape (bundle branch blocks, extrasystolas) pathologic Q (myocardial infarction)
Spikes and waves analysis ST interval– isoelectric pathology – elevation, depression
Spikes and waves analysis Wave T – repolarization of ventricles coronary T hyperkalemia hypokalemia
Spikes and waves analysis Interval QT – prolongation: hypocalcemia hypokalemia - shortening: hypercalcemia hyperkalemia digitalis toxicity
Right ventricular hypertrophy • right axis deviation • signs of cardiac overload • right bundle branch block • P-pulmonale
Left ventricular hypertrophy left axis deviation voltage criteria: Sokolow-Lyon index S in V1 + R in V5 or V6 (whichever is larger) ≥ 35 mm Lewis index R I + S III ≥ 25 mm
Left ventricular hypertrophy with signs of cardiac overload overload - descendent depression of ST and negative T in I, aVL, V5 and V6
Current of injury Current of injury Current of injury Current of injury Ischemic changes in ECG, myocardial infarction
Initial ECG classification of myocardial infarction STEMI „ST elevation MI“ NSTEMI „nonST elevation MI“
NSTEMI - subendocardial ischemia descendent depression of ST 0.08 s in width and 1 mm in amplitude
NSTEMI subendocardial ischemia coronary T wave, ST depression
STEMI – myocardial infarction pathologic Q wave deflection amplitude of 1/4 or more of the subsequent R wave or being > 0.04 s in width and > 2 mm in amplitude ST elevation negative T
STEMI – anterior wall myocardial infarction Pardee wave (elevation of ST)
reentry ARRHYTMIAS • Mechanisms of arrhytmias: • Abnormal impulse formation • Abnormal conduction • 3. Combination of both • - irregular heartbeat • tachyarrhytmia – rate > 100/min • bradyarhytmia – rate < 60/min
Incomplete compensatory pause (supraventricular arrhytmia) Complete compensatory pause (ventricle extrasystole)
Nodal rhytm absence of P waves
WPW syndrome (Wolf-Parkinson-White) ventricular pre-excitation PQ 0,12 s typical delta wave
Atrial fibrilation irregullar formation of impulses in atria 300-600/min irregular QRS complexes absence of P waves flutter like waves f
Atrial flutter atrial rate of 240 to 340 beats/minute repeated loop of electrical activity sawtooth pattern of the P waves
Premature ventricular complexes PVCs (extrasystoles) ectopic impulses originating from an area distal to the His Purkinje fibres unifocal PVCs are triggered from a single site in the ventricle complexes have different configurations >0,11s in width is usually followed by a complete compensatory pause
Premature ventricular complexes – ventricular bigeminy Depending whether there are 1, 2, or 3 normal beats between each PVC, the rhythm is called bigeminy, trigeminy, or quadrigeminy Causes: high blood pressure, low blood oxygen, low blood levels of potassium, and some medications (digitalis toxicity)
Ventricular tachycardia series of three or more ventricular complexes occurring at a rate of 100 to 250 bpm atrioventricular dissociation is usually seen wide QRS complexes (usually >120 ms) with T-wave polarity opposite that of the major QRS deflection;
Ventricular fibrillation abnormally irregular heart rhythm caused by rapid, uncoordinated fluttering contractions of the ventricles mechanically this results in an arrested cardiac pump function and immediate death
First-degree atrioventricular block PR constant prolongation disease of the conduction system in which the PR interval is lengthened 0.20
Second-degree AV block Type 1Mobitz I/ Wenckebach periodicity almost always a disease of the AV node is characterized by progressive prolongation of the PR interval on consecutive beats followed by a blocked P wave (i.e., a 'dropped' QRS complex) pattern n: (n-1)
Second-degree AV block Type 2Mobitz II intermittent non-conducted P waves without progressive prolongation of the PR the P waves ‘march through’ at a constant rate
Third degree AV block complete heart block the atrial activity is dissociated from ventricular activity regular P to P interval, regular R to R, clinically: bradycardia, hypotension, hemodynamic instability
Right bundle branch block defect in the heart's electrical conduction system the right ventricle is not directly activated by impulses travelling through the right bundle branch QRS duration must be more than 100 ms (incomplete block) or more than 120 ms (complete block) terminal R wave in lead V1 (e.g. R, rR', rsR', rSR' or qR)
Leftt bundle branch block activation of the left ventricle is delayed QRS duration must be ≥ 0.12 s should be a QS or rS complex in lead V1 RsR' wave in lead V6.
Přehled svodů užívaných v EKG I - + aVR aVL - - II III + + uzemnění aVF 12 – ti svodové EKG: • 3 bipolární končetinové svody I, II, III tzv. Einthovenův trojúhelník • 3 unipolární zesílené svody aVR, aVL, aVF proti Goldbergově svorce • 6 unipolárních hrudních svodů V1-6 proti Wilsonově centrální svorce