Download
1 / 22
220 likes | 505 Views
Pediatric Critical Care Telemedicine in Community Emergency Departments. David McSwain, MD MPH Pediatric Critical Care Medicine Medical Director, MUSC Inpatient and Emergency Teleconsultation. Access to Subspecialty Care.

E N D
Pediatric Critical Care Telemedicine in Community Emergency Departments David McSwain, MD MPH Pediatric Critical Care Medicine Medical Director, MUSC Inpatient and Emergency Teleconsultation
Access to Subspecialty Care • Only 3% of pediatric critical care physicians practice in rural areas. • The vast majority of ED visits by children are made to general hospitals.1 • Children make up 27% of all ED visits nationwide. • Only 6% of ED’s in the US have all the necessary pediatric supplies. • Only half have even 85% of necessary supplies. • Critically ill patients transferred from outlying facilities have worse outcomes (mechanical ventilation, inotropes, PICU length of stay) compared to patients admitted from the same facility.2 Institute of Medicine. 2006. Academic Emergency Medicine. 13(10) Gregory et al. 2009. Pediatrics. 121(4): e906-e911
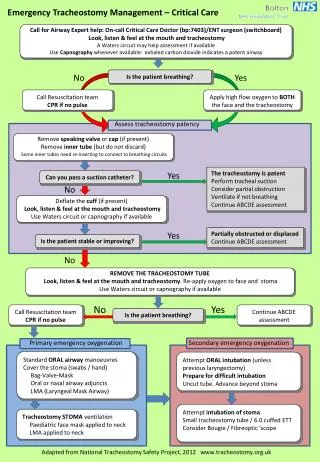
The Problem • Hours can elapse from the time a community facility calls for assistance and the time a subspecialist sees a critically ill child. • Assessing the acuity of injury or illness and determining appropriate pre-transfer interventions in a child over the telephone is at times extremely difficult. • This can create an extraordinarily stressful experience for the patient, patient’s family, and the involved providers.
MUSC Pediatric Emergency and Critical Care Telemedicine Program (PECCT) • $525,943 Duke Endowment grant for three years • Pediatric emergency medicine and critical care physicians will be available 24/7 through the telemedicine program. • Program designed to serve as foundation for future telemedicine programs • Utilizes standard communication platforms to maximize adaptability • Focusing on integrating existing telemedicine programs at MUSC into a unified system • Goal is to optimize the ease of implementation for new and developing programs
Pilot Facilities Waccamaw Community Hospital Conway Medical Center
Pilot Facility Status • Conway • Utilized credentialing-by-proxy • Program fully implemented in May 2014 • Georgetown/Waccamaw • Initially used traditional credentialing • Now proceeding with credentialing-by-proxy • Revision of hospital bylaws pending • Colleton • Utilizing traditional credentialing • Credentialing still in progress
Referral/Transfer Data • Collecting data on all calls for pediatric emergency medicine or critical care for transfer or consultation. • Since April 2012 • 776 records • 432 surveys completed • 424 did not use telemedicine • 8 used telemedicine
Location at Referring Site 633 (89.5%) 28 (4.0%) 21 (3.0%) 16 (2.3%) 9 (1.3%)
Patient Transferred to MUSC? • 25 transported patients (7.3%) could have been managed at referring facility • 8 telemedicine consults • 1 patient not transferred (12.5%) • Facial burn. Would have been transferred if not for telemedicine. • The following is NOT statistically significant!! • NNT to avoid one transport: 9.5 98.0% 2.0%
Initial Transport Destination • 23 (10.5%) non-TM patients could have been triaged to a lower level of care • 12 to Intermediate • 11 to Floor • Three of eight telemedicine patients transferred to PICU • 1 not transferred • 3 to MUSC ED (then floor) • 1 to Intermediate • All triage decisions felt to be appropriate in retrospect • Use of telemedicine influenced triage decision in 50% of cases 37.4% 47.1% 13.5% 2.1%
Transportation • Helicopter: 27.6% • Ground because unable to fly: 9.5% • Ground: 58.4% • Fixed-wing: 0.7% • Private Vehicle: 3.8% • Incorrect mode of transport for 25 patients (6.5%) • Five ground transports should have gone via air • 17 air transports should have gone by ground • Telemedicine consults: 3 ground, 1 unable to fly, 3 helicopter • All three ground transports would have been by helicopter if not for telemedicine • All transport decisions judged to be appropriate in retrospect
Telemedicine Quality Scale: 1 = “very poor”, 5 = “excellent” • In all eight cases, examiners stated that telemedicine “improved” (2) or “greatly improved (6) the overall quality of the initial consult.
Telemedicine Vignettes • Teenager with near-drowning • Gathered information during arterial line placement by ED physician • Infant with SVT • Diagnosis and management with cardiology fellow • Toddler with AMS • Directly observed lumbar puncture • Teenager with rash and fever • Ruled out TSS and confirmed stability for intermediate care • Toddler with ataxia • Lengthy discussion with parents involving PICU and ED physicians • Child with facial burn • Management recommendations provided and child discharged home
Access to Subspecialty Care • Percent of population below poverty level • Georgetown County: 21% • Horry County: 22% • Colleton County: 21% • Percent of pediatric patients hospitalized at MUSC • Georgetown County: 28% • Horry County: 24% • Colleton County: 51% • ED/PICU calls September 1, 2012 – August 31, 2013 • Georgetown Memorial Hospital: 37 • Waccamaw Medical Center: 32 • Colleton Medical Center: 33 • Conway Medical Center: 24 • All facilities: 467 • Four pilot facilities accounted for 27% of calls • Number not transferred: 25 (5%)
Referral Sites McLeod Health - Florence (20, 2.6%) Moncks Corner Medical Center (22, 2.8%) NasonMedical Center (9, 1.2%) Orangeburg Regional Hospital (11, 1.4%) Palmetto Health Richland (10, 1.3%) Roper Berkeley Day Hospital (21, 2.7%) Southstrand Ambulatory Care (9, 1.2%) Summerville Medical Center (93, 12.0%) Trident Medical Center (47, 6.1%) Waccamaw Medical Center (47, 6.1%) Williamsburg Regional Hospital (8, 1.0%) Coastal Carolina Medical Center (8, 1.0%) • Beaufort Memorial Hospital (78, 10.1%) • Bon Secours Saint Francis Hospital (16, 2.1%) • Clarendon Memorial Hospital (12, 1.6%) • Colleton Medical Center (39, 5.1%) • Conway Medical Center (48, 6.2%) • East Cooper Regional Medical Center (16, 2.1%) • Georgetown Memorial Hospital (49, 6.3%) • Grand Strand Regional Medical Center (51, 6.6%) • Greenville Memorial Hospital (14, 1.8%) • Hampton Regional Medical Center (11, 1.4%) • Hilton Head Medical Center and Clinics (15, 1.9%)