Download
1 / 43
520 likes | 1.15k Views
OSTEOSARCOMA- Case Presentation: At- Shaheed-Suhrawardy-Medical-College-Hospital-Dhaka-Bangladesh

E N D
Case Presentation ON A Young Girl With Hard Mass At The Distal 3rd Of Lt. Thigh.
From Department Of Orthopedic & Traumatology, ShaheedSuhrawardyMedical College Hospital, Dhaka-1207. Bangladesh. Presenting By- Dr. GolamMuhamud (Suhash). Prepared By- Dr. Md Nazrul Islam MBBS, M . sc. (B M E).
Particulars of the patient: Name :Ms. Fatema Age :18years Sex :Female Address: 236, Ahmednagar, Mirpur, Dhaka. Marital status- Married Date of admission: 15-09-2010 Date of examination:16-09-2010
Chief complaints: • Pain just above the left knee joint for 3 months. • Swelling above the left knee joint for 2 months. • Inability to walk for 1 month.
Present illness- • According to the statement of the patient she was reasonably well 3 months back. Then she suddenly developed mild, fixed, aching pain just above the left knee joint which was not associated with fever. • Pain is non-radiating, aggravated during walking and worse at night and partially relieved by taking NSAIDS.
Present illness- • Two months back she also noticed swelling above left knee joint associated with pain which was initially small in size then increasing rapidly to a large . She has no history of trauma. • In addition to swelling there is a sudden deformity of the left knee from last 1 month and patient can not move her knee freely or walk without support.
Present illness- • She has h/o wt. loss, and loss of appetite but she has /had no complaints of pain, swelling and deformity in other parts of the body. She has no history of cough , haemoptysis, DM , HTN and asthma. • With these complaints she got herself admitted into ShaheedSuhrawardy Medical college Hospital for better management.
past illness- • She had no history of tuberculosis. Drug history: • H/O taking analgesic for 3 months but could not mentioned the name of drugs.
Family history- Personal history: Nothing contributory None of her family member suffered from such illness.
Menstrual history- • MP-4 to 6 days • MC-regular • Age of menarche-13yrs.
Immunization History: Socio-economic History- Poor Immunized against – Tuberculosis & Tetanus
General Examination- • Appearance- Ill looking • Body builds- Below average • Co-operation- Co-operated • Decubitus- Supine • Anaemia- Moderate • Jaundice- Absent • Cyanosis- Absent • Clubbing- Absent • Koilonychia-Absent • Lekonychia- Absent • Lymph nodes- Not palpable • Dehydration- No sign • Pulse - 84 Beat/min • Blood pressure- 100/60mm of Hg • Temperature-normal • Respiratory rate-16/min
Local Examination(left lower limb): • An ill-defined diffuse swelling occupying at the supracondylar area of left thigh. • Skin is shiny with presents of engorged vein. • Flexion deformity of knee with shortening of the lower limb. • Unable to walk without support. • Wasting of the thigh and leg with fullness of patellar hollow. Look-
Local Examination(left lower limb).(cont). Feel- • There is an ill defined diffuse swelling extending from the lower pole of the patella to the supracondylar region of femur and diffusely enlarged medially and laterally and back of the upper part of knee. • Size of swelling is (12x10)cm.Local temperature- raised ,surface -smooth, margin- ill-defined, tenderness present, over lying skin is free, consistency- hard, not movable and fixed with underlying structure.
Local Examination(left lower limb). cont. • Fluctuation test- negative, • Trans-illumination test-negative, • Patellar tap test- negative. • Shortening of limb - 3 cm. • Muscle wasting- Thigh – 4 cm. Leg – 2 cm • Distal neurovascular status- normal • Regional lympnodesnot enlarged.
Local Examinationleft lower limb (cont.) Movement: • walk with support. • Left knee (ROM)– • Active flexion -Absent • Active extension-Absent • Patellar movement-Absent • Left hip & ankle: normal range of movement
Systemic examination: Locomotor system Gait: Can walk with support Inspection: Flexion attitude- Left knee(20 degree) Palpation: Tenderness – affected area. Spine: Normal
Nervous system examination: • Higher psychic function: Normal • Cranial Nerve examination: Normal • Motor function: Inspection: Gross Muscle wasting in left thigh & leg.
Nervous system examination: • Palpation: • Bulk of muscle wasting: Left thigh-4cm,left leg- 2cm. • Tone of muscle: Muscle tone is normal
Nervous system examination: Power: [MRC scale]: Normal but muscle power could not elicited around left knee due to pain and deformity.
Nervous system examination: • Deep tendon reflex: All jerks are present & normal • Sensory function test: All the sensory functions are normal.
Respiratory system examination: • Inspection: Normal in size & shape of the chest- Respiratory rate: 16 /min • Palpation: Trachea centrally placed, normal chest expansibility • Percussion: Resonant all over the chest except right upper, middle and lower zone where dullness is present. • Auscultation: Bronchial breathing sound with diminished breathing sound in Rt. Upper middle and lower zone.
Cardiovascular system examination: • Pulse: 84 bts/ min • B.P. 110/60 mm of Hg • JVP: Not raised. • Inspection: NAD • Palpation: Apex beat in Lt 5thintercostal space, • Percussion: superficial cardiac dullness presence over the precordium. • Auscultation: s1 & s2 is audible
Alimentary system: examination: • Inspection: nothing abnormality detected • Palpation: soft, non tender • Percussion: tympanic • Auscultation: bowel sound present • Per-rectal examination: normal findings.
Salient feature: Ms. Fatema, 18 years ill-looking, moderately anaemic, non icteric, nondiabetic, normotensive woman coming from Mirpur, Dhaka admitted in ShaheedSuhrawardy Medical College Hospital with thecomplaints of – • pain, just above the left knee joint 3 months back , • swelling above the left knee joint 2 months back and • inability to walk for 1month.
Salient feature: • The pain was initially mild , fixed, non radiating, aching in nature but gradually it becomes intolerable which was aggravated during walking and worse at night & incompletely relived by taking NSAIDs.Thispain was not associated with fever. • She also noticed an ill defined swelling above left knee joint which was initially.
Salient feature: Small in size then it increases rapidly to a large size.It is associated with pain but not related to trauma. • She also gives H/O inability to walk due to pain,swelling and restriction of movement. • She gives H/O wt loss,loss of appetite but she has no H/O pain,swelling,deformity in other parts of body.
Salient feature: • On local examination- an ill defined diffuse swelling occupying over the supracondylar region of the left thigh with shiny skin and presents of engorged vein and wasting of the thigh and leg. • She has a deformity of knee and cannot walk without support.
Salient feature: • The surface of swelling smooth, margin- ill-defined, local temperature-raised , tenderness present, over lying skin is free, consistency-hard, not movable and fixed with underlying structure. • Shortening of the left limb was found 3 cm than the right. She was unable to walk without support.
Salient feature: • There was gross muscle wasting in left Lower limb, measuring thigh- 4cm, leg- 2 cm. • Neuromuscular status of left lower limb normal and regional lympnodes are not enlarged.Movement of the left knee joint absent hip and spine are normal. • On respiratory system examination-there was a dullness in Rt upper and lower zone of lung and breath sound also diminished in same area.Other system examination reveals no abnormality.
Provisional Diagnosis: Osteosarcoma - With pathological fracture at supra-Condylar region of left femur.
Differential diagnosis • Ewing’s sarcoma • Chronic osteomyelitis with pathological fracture. • Aneurysmal bone cyst with pathological fracture. • Giant cell tumor with pathological fracture.
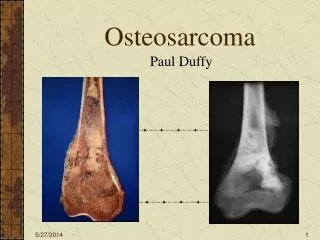
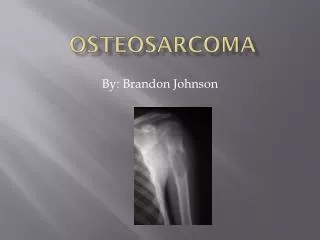
Investigation: X-Ray- Left knee including part of the thigh and leg A/P and lateral view shows-hazy osteolytic and osteoscleroticleison along with fracture occupying at lower end of femur. The edo-osteal margin poorly defined,cortex breached with soft tissue involvement.
X-ray left knee including part of the thigh and leg A/P and lateral view: Investigation:
Heart-no abnormalityLungs-hazziness in Rt. upper and lower zone at Rt. costo-diaphramatic angle is obliterated and small hazziness in the left middle zone. Investigation: X-ray chest P/A view:
CT scan of left lowerlimb- • Extensive bone destruction is seen in the left lower femoral shaft, condyles and tibialcondyles with soft tissue extension. • peripheral calcification also seen. • Bone destruction also seen in L5 vertebra.
Investigation: CT Scan of Lt. Lower Limb & Lungs- Multiple metastatic nodules in both lungs along with Rt. Sided Hydro-pneumothorax-
Investigation: • Blood- • TC of WBC 14800 / cu mm • DC of WBC • N 75%B 00% • L 20%M 05% • E 02% • ESR 65 mm in 1st hr . • Hb% 8.40 gm / dl. • Urine- RME - Normal study. • RBS : 5.85mmol/lt.
Investigation: • S. creatinine 0.6 mg/ dl • Blood urea 30 mg / dl • S. calcium 7.5 mg / dl • S. alkaline phosphates 110 IU/ L • SGPT:26 IU/L , SGOT :33 IU/L • S. bilirubin:1.0 mg/dl • FNACSarcomatousleison,suggestive of osteosarcoma. • Biopsy (incisional): Feature of osteosarcoma with osteod formation and many giant cells.
ConfirmatoryDiagnosis: Osteosarcoma With pathological fracture at the lower end of lt. femur (stage -III).
Management/ Treatment: Palliative treatment given: • For fracture- plaster / immobilization • For pain- NSAIDS. • Bis- phosphonate . As it is a malignant tumor with stage-III- Our next plan- • Consultation with oncologist for neo-adjuvant chemo / radiotherapy then- 2. Mid-thigh amputation.
Thank You AllFrom -Department Of Orthopedic & Traumatology, Shaheed Suhrawardy Medical College Hospital For Patience& Attention.