Download
1 / 44

E N D
atypical facial pain • SYMPTOMSFacial pain, often described as burning, aching or cramping, pulling, occurs on one side of the face, often in the region of the trigeminal nerve and can extend into the upper neck or back of the scalp. Although rarely as severe as trigeminal neuralgia, facial pain is continuous for ATFP patients, with few, if any periods of remission.
DIAGNOSISDiagnosing atypical facial pain is not an easy task. It's not unusual for ATFP patients to have undergone numerous dental procedures, seen multiple doctors and undergone many medical tests before being successfully diagnosed and treated. A diagnosis of ATFP is usually a process of elimination. When a patient complains of constant facial pain restricted to one side of the face, the physician must first rule out any other conditions. Tests include roentgenograms of the skull, MRI and/ or CT scan with particular attention to the skull base, careful dental and otolaryngolgic evaluation, and thorough neurological examination. Only after tests rule out other factors can a diagnosis of ATFP be made.
TREATMENTSTreatment of ATFP can be difficult and perplexing for both doctor and patient. Medication is usually the first course of treatment. Surgical procedures such as microvascular decompression generally are not successful with ATFP patients. The following drugs are used to treat atypical facial pain: Amitriptyline. (Triptyl, Elavil) Gabapentin. (Neurontin). Pamelor Capsaicin Other pain relief strategies include: Hot and cold compresses Acupuncture
Atypical odontalgia • Atypical odontalgia describes atypical facial pain in apparently normal teeth. Unfortunately, dentists usually consider this diagnosis only after the failure of invasive treatment. Atypical odontalgia patients are typified by women in their mid-40s who complain of persistent pain in one or more premolar or molar teeth. They associate pain with dental procedures or trauma to the region, While the cause of atypical odontalgia is uncertain.
Patients with unrelenting pain in the teeth, gingival, palatal or alveolar tissues often see multiple dentists and have multiple irreversible procedures performed and still have their pain. Up to one-third of patients attending a chronic facial pain clinic have undergone prior irreversible dental procedures for their pain without success. In these cases, if no local source of infectious, inflammatory, or other pathology can be found, then the differential diagnosis must include a focal neuropathic pain disorder.
The common diagnoses given include the terms atypical odontalgia, persistent orodental pain, or if teeth have been extracted, phantom tooth pain. One possibility is that these pain complaints are due to a neuropathic alteration of the trigeminal nerve. There are several diagnostic procedures that need to be performed in any patient suspected of having a trigeminal neuropathic disorder including (1) cold testing of involved teeth for pulpal nonvitality; (2) a periapical radiograph examining the teeth for apical change; (3) a panoramic radiograph examining for other maxillofacial disease; (4) a thorough head and neck examination also looking for abnormality; (5) a cranial nerve examination including anesthetic testing which documents any increased or decreased trigeminal nerve sensitivity and rules out other neurologic changes outside the trigeminal nerve; and (6) MRI imaging in some cases
Finally, when a nonobvious atypical toothache first presents, direct microscopic examination of the tooth for incomplete tooth fracture is also suggested. The majority of these patients are women over the age 30 with pain in the posterior teeth/alveolar arch. Multiple causes exist for sustained neuropathic pain including direct nerve injury (e.g., associated with fracture or surgical treatment), nerve injection injury, nerve compression injury (e.g., implant, osseous growth, neoplastic invasion) and infection-inflammation damage to the nerve itself. Sustained nerve pain is commonly seen in patients with psychiatric impairment. It may be that the unrelenting nature of the pain itself alters the patient's personality.
Treatment includes pharmacologic medications which suppress nerve activity. The common medications used for atypical odontalgia and phantom tooth pain include gabapentin, tricyclics, topical anesthetics, and opioids.. With earlier treatment, better pain control and this should also prevent secondary psychiatric disease from developing and lower the number of inappropriate treatments
What is Atypical Odontalgia? • Atypical Odontalgia (AO) is a condition in which a tooth is very painful but nothing can be found wrong with the tooth. The pain is continuous, usually burning, aching and sometimes throbbing and most often occurs in upper premolars (bicuspids) or molars.Since symptoms are very similar to those caused by a "toothache", often numerous dental procedures are done.To complicate matters, these treatments (such as pulp extirpation, root-tip surgery or tooth extraction) may offer temporary relief from pain, only to have the pain return.
What are the Signs & Symptoms of Atypical Odontalgia? • The typical clinical presentation of AO involves pain in a tooth in the absence of any sign of pathology; the pain may spread to areas of the face, neck, and shoulder.Symptoms include a continuous burning, aching pain in a tooth or in the bone / gum surrounding a tooth.Often there in increased sensitivity to pressure over the painful region. Often nothing shows up on diagnostic tests, no abnormalities are found on X-rays and no obvious cause for the “tooth pain” can be found.Patients often have difficulty localising the pain.All ages can be affected except for children. AO seems to be more common in women in their mid 30 - 40’s.Diagnosis is based primarily on symptoms and on elimination of other possible disorders. Tests may include diagnostic dental X-rays, CT scans and possibly MRI scans. If a nerve block does not result in pain reduction then a diagnosis of AO should be considered
How is it treated? • Medications such as painkillers and sedatives are not effective in AO. Surgery and other dental interventions rarely provide relief.Anti-depressants medications can reduce AO pain which is probably due to their analgesic effects (Anti-depressantshave the ability to produce low-grade pain relief at lower strengths) and not to their anti-depressant effects. AOpatients are generally not depressed.Topical application of capsaicin to painful tissue has also been investigated as a treatment for AO.The outcome is usually fair, with many patients obtaining complete relief from pain.Especially in the absence of overt pathology, particular attention should be paid to avoiding any unnecessary and potentially dangerous dental intervention on the teeth.AO is surprisingly common, of uncertain origin and potentially treatable.
Dysgeusia • Dysgeusia is the medical term for an altered, distorted or reduced ability to taste. • Specific types of taste disorders include hypogeusia (a reduced ability to taste) and ageusia (an inability to detect taste). A persistent bad taste in the mouth (parageusia) is sometimes used interchangeably with dysgeusia.So Distortion may include sensing a taste that is not present in the mouth, or misidentifying a taste (e.g., pleasant-tasting foods now taste awful).
The sense of taste begins in the mouth. A person is born with approximately 10,000 taste buds, most of which are located on or around the papillae of the tongue. Taste buds are also located on the soft palate, pharynx , larynx , epiglottis and the first part of the esophagus
Each taste bud contains anywhere from 50 to 100 taste cells. Each of these cells responds best to one of five basic taste sensations: Sweet (e.g., sugar) Sour (e.g., lemon juice) Salty Bitter (e.g., aspirin) Umami (sometimes spelled umame) or “savory”
When stimulated, a taste cell sends a nerve impulse to the brain, where a certain taste is identified and sensed. New taste cells are constantly being produced by the body, replacing existing taste cells every 10 days throughout a person’s life. Thus, if taste cells are destroyed by burning the mouth with a hot liquid, any consequent taste disorder is usually temporary, until new taste cells are produced .For complex tastes, the sense of smell is required. Many taste disorders are actually associated with an impaired sense of smell (dysosmia), which can occur due to colds or other upper respiratory infections. Often, people do not discover they have a smell disorder until they notice a problem with taste.
More than 200,000 people seek help for a taste or smell disorder every year, according to the National Institutes of Health. The actual incidence of these disorders is estimated to be in the millions because a large number of people do not seek help for the condition. Taste disorders can affect a person’s quality of life. It can lead to a decreased appetite, poor nutrition and the inability to identify potentially harmful foods or beverages
Taste disorders can have many different causes. Various illnesses (e.g., colds, sore throat), lifestyle habits (e.g., smoking), irritants (e.g., insecticides, certain prescription mouthwash) and other factors (e.g., medications) can contribute to dysgeusia. Patients are urged to contact their physician or dentist if they have a taste disorder that lasts two weeks or longer. A thorough medical history may be taken, including questions about symptoms, current medications and medical conditions, recent illnesses, and whether the patient’s sense of smell is affected.
. Tests that measure the extent of a person’s sense of taste or smell may be performed. If no underlying medical or dental condition is identified, the patient may be referred to a facility that specializes in taste and smell disorders. The physician, dentist or other healthcare provider will attempt to identify the underlying cause of a patient’s dysgeusia. How symptoms of dysgeusia begin can help indicate the underlying cause. For instance, a sudden loss of taste may be due to trauma or a severe upper respiratory infection. For dysgeusia that occurs off and on, an allergy or exposure to chemicals may be the cause.
Treatment of dysgeusia depends on its cause. Typically, treating the underlying condition will also eliminate the patient’s dysgeusia. The prognosis for patients is generally excellent when the cause of dysgeusia can be identified and treated. However, long-term recovery is more complicated when the source of dysgeusia cannot be identified or when dysgeusia results from an untreatable condition. For the most part, dysgeusia cannot be prevented. However, quitting smoking, practicing good oral hygiene, having regular dental examinations and treating sinus problems all can contribute to reducing the likelihood of dysgeusia.
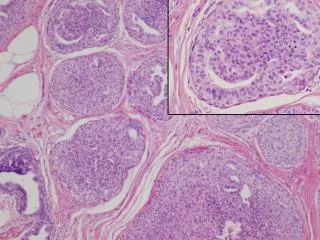
SALIVARY GLAND ANATOMY ANDPHYSIOLOGY • There are three major salivary glands: parotid, submandibular, • and sublingual. These are paired glands that secrete a highly • modified saliva through a branching duct system. Parotid • saliva is released through Stenson’s duct, the orifice of which • is visible on the buccal mucosa adjacent to the maxillary first • molars. Sublingual saliva may enter the floor of the mouth via • a series of short independent ducts, but will empty into the • submandibular (Wharton’s) duct about half of the time. The • orifice of Wharton’s duct is located sublingually on either side • of the lingual frenum. There are also thousands of minor salivary • glands throughout the mouth, most of which are named • for their anatomic location (labial, palatal, buccal, etc). These • minor glands are located just below the mucosal surface and • communicate with the oral cavity with short ducts.
Saliva is the product of the major and minor salivary glands dispersed throughout the oral cavity. It is a highly complex mixture of water and organic and non-organic components.. The three major salivary glands share a basic anatomic structure. they are composed of acinar and ductal cells arranged much like cluster of grapes on stems. The acinar cells make up the secretory end piece. those of the parotid gland are serous, those of the sublingual gland are mucous, and those of the submandibular gland are of a mixed mucous and serous type. The duct cells (the “stems”) form a branching system that carries the saliva from the acini into the oral cavity. The duct cell morphology changes as it progresses from the acinar junction toward the mouth .
proteins are produced and transported into the saliva through both acinar and ductal cells. The primary saliva within the acinar endpiece is isotonic with serum but undergoes extensive modification within the duct system, with resorption of sodium and chloride and secretion of potassium. The saliva, as it enters the oral cavity, is a protein-rich hypotonic fluid. The secretion of saliva is controlled by sympathetic and parasympathetic neural input.
xerostomia • called "dry mouth," among patients who take medications, have certain connective tissue or immunological disorders or have been treated with radiation therapy. When xerostomia is the result of a reduction in salivary flow, significant oral complications can occur.
Xerostomia often develops when the amount of saliva that bathes the oral mucous membranes is reduced. However, symptoms may occur without a measurable reduction in salivary gland output. The most frequently reported cause of xerostomia is the use of xerostomic medications. A number of commonly prescribed drugs with a variety of pharmacological activities have been found to produce xerostomia as a side effect. Additionally, xerostomia often is associated with Sjögren’s syndrome, a condition that involves dry mouth and dry eyes and that may be accompanied by rheumatoid arthritis or a related connective tissue disease. Xerostomia also is a frequent complication of radiation therapy.
Xerostomia is an uncomfortable condition and a common oral complaint for which patients may seek relief from dental practitioners. Complications of xerostomia include dental caries, candidiasis or difficulty with the use of dentures. The clinician needs to identify the possible cause(s) and provide the patient with appropriate treatment
Xerostomia is defined as a subjective complaint of dry mouth that may result from a decrease in the production of saliva. Xerostomia is estimated to affect millions of people in the United States. Studies have found the condition in 17 to 29 percent of sampled populations based on self-reports or measurements of salivary flow rates. Complaints of dry mouth generally are more prevalent in women
its diminution or absence can cause significant morbidity and a reduction in a patient’s perceptions of quality of life. The primary constituents of saliva are water, proteins and electrolytes. These components enhance taste, speech and swallowing and facilitate irrigation, lubrication and protection of the mucous membranes in the upper digestive tract Additional physiological functions of saliva provide antimicrobial and buffering activities that protect the teeth from dental caries.
.Patients initially may be unaware that a reduction in salivary flow is occurring unless some of its complications, such as an increase in cervical dental caries, becomes apparent. Only after the development of symptoms—which may include soreness, burning or difficulty with swallowing—is the patient likely to seek relief from the practitioner
physiopathology • Saliva is produced by the parotid, submandibular and sublingual glands, as well as by hundreds of minor salivary glands that are distributed throughout the mouth. Daily salivary output is estimated to be approximately one liter per day, Salivary flow is categorized as unstimulated, or resting, and stimulated, as occurs when an exogenous factor is acting on the secretory mechanisms • Both the parasympathetic and sympathetic nervous systems innervate the salivary glands. Parasympathetic stimulation induces more watery secretions, whereas the sympathetic system produces more viscous flow. Therefore, a sensation of dryness may occur, for example, during episodes of acute anxiety or stress, which cause changes in salivary composition owing to predominant sympathetic stimulation during such periods.
causes • Medications. Xerostomia is a common and significant side effect of many commonly prescribed drugs.. Nevertheless, the risk for xerostomia increases with the number of drugs being taken. Older people, therefore, are more likely to be affected. In the geriatric population, drug-induced xerostomia has been reported to contribute to difficulty with chewing and swallowing; this may result in avoidance of certain foods. • A variety of drugs that have a wide range of therapeutic activities have been reported to cause xerostomia in 10 percent or more of patients. Drug-induced hyposalivation also can be an extension of the drug’s intended action, as seen with the parasympatholytic agents (such as atropine), or as an anticholinergic side effect with drugs such as tricyclic antidepressants.
Sjögren’s syndrome. When xerostomia is associated with xerophthalmia, also known as "dry eyes," it may represent a chronic autoimmune condition that is recognized as Sjögren’s syndrome, which affects predominantly women after the fourth decade of life. In primary Sjögren’s syndrome, the disease is limited to the eyes and salivary glands. With secondary Sjögren’s syndrome, patients also have an autoimmune or connective tissue disease .It is estimated that 15 percent of patients with rheumatoid arthritis, 25 percent of those with systemic sclerosis and 30 percent of those with systemic lupus erythematosus may develop Sjögren’s syndrome.
The xerostomia that is associated with primary and secondary Sjögren’s syndrome has been attributed to the progressive lymphocytic infiltration that gradually destroys the secretory acini of the major and minor salivary glands. Another explanation for the loss of glandular function may be related to an inhibition of nerve stimuli of the glands. It has been suggested that the reduction in secretions first may affect the minor salivary glands, which can initiate the symptoms of xerostomia.
Radiation therapy. Radiation therapy of the head and neck regions is employed as a primary, concomitant or adjuvant treatment modality for primary and recurrent tumors in the upper aerodigestive tract.. Ionizing radiation can injure the major and minor salivary glands; this can lead to atrophy of the secretory components and result in varying degrees of temporary or permanent xerostomia
Other conditions. Diseases with immunological abnormalities other than autoimmunity may be accompanied by Sjögren’s-like manifestations or xerostomia .Infection with HIV has been associated with arthritis, parotid gland enlargement and xerostomia. Xerostomia has been reported in 45 to 60 percent of patients who did allogenic bone marrow transplantation. Loss of saliva and a number of immunological abnormalities also have been implicated as possible complications of silicone breast implants. Patients undergoing hemodialysis for end-stage renal disease have developed dry mouth and reduced salivary gland function, but these manifestations may be attributed in part to medications being used to treat coexisting conditions. Anxiety, depression or stress also may give rise to subjective symptoms of dry mouth.Patients with diabetes mellitus, particularly those who have poor glycemic control, are more likely to complain of xerostomia and may have decreased salivary flow.
Clinical manifestation • A reduction of saliva may lead to complaints of a dry mouth, oral burning or soreness or a sensation of a loss of or altered taste. Another manifestation may be an increased need to sip or drink water when swallowing, difficulty with swallowing dry foods. Patients who develop Sjögren’s syndrome secondary to a connective tissue disease also may complain of having dry eyes, and progressive parotid gland enlargement may become evident. These initial manifestations may precede clinically apparent alterations of the oral mucosa or any measurable reduction in salivary gland function. As the xerostomia progresses, inspection of the oral cavity may disclose an erythematous, cobblestoned or fissured tongue and atrophy of the filiform papillae. Palpation of the oral mucosa may result in the finger’s adhering to the mucosal surfaces instead of readily sliding over the tissues. Application of a dry cotton swab at the parotid and sub-mandibular duct orifices followed by external palpation of the glands may reveal delayed or inapparent salivary flow from the ducts.
Dental-related findings include evidence of an increased tendency to develop cervical caries and denture discomfort accompanied by loss of retention. Lack of saliva increases susceptibility to infection of the oral cavity and oropharynx by the opportunistic fungus Candida albicans, or thrush. Manifestations of oral infection with Candida include erythema of the oral mucosa; white, and inflamed fissures at the corners of the mouth, a condition called cheilitis
diagnosis • An affirmative response to at least one of the five following questions about symptoms has been shown to correlate with a decrease in saliva: "Does your mouth usually feel dry? Does your mouth feel dry when eating a meal? Do you have difficulty swallowing dry foods? Do you sip liquids to aid in swallowing dry foods? Is the amount of saliva in your mouth too little most of the time, or don’t you notice it
A number of supplemental tests are available that can be used to confirm the subjective manifestations of xerostomia. Salivary output can be measured, and a collected amount of less than 0.12 to 0.16 milliliters per minute (unstimulated) has been suggested to be the criterion for hypofunction. Imaging modalities, including sialography and scintigraphy, also have been used to examine salivary gland function. Criteria for the clinical, laboratory and histopathologic manifestations that are consistent with a diagnosis of Sjögren’s syndrome recently were revised
MANAGEMENT • The general approach to treating patients with hyposalivation and xerostomia is directed at palliative treatment for the relief of symptoms and prevention of oral complications. • If the patient’s xerostomia is caused by the side effect of a drug, the dentist can recommend an alternative medication, but this course may not be beneficial if the alternate drug has a mode of action similar to that of the original drug. Modification of the dosage regimen is another strategy that may increase salivary flow. The practice of carrying and sipping bottled water throughout the day, which has become popular, also may offer relief for affected patients. When at home, the patient can hold ice chips in his or her mouth to provide moisture and possibly alleviate symptoms.
A number of products that can function as saliva substitutes have been developed specifically for patients with xerostomia. Available in a variety of formulations—including rinses, aerosols, chewing gum and dentifrices these products also may promote salivary gland secretions. incorporation of metal in the palate of the maxillary denture have been shown to be beneficial treatment options for some patients.
MANAGEMENT OF HYPOSALIVATION AND XEROSTOMIA.The use of parasympathomimetic drugs such as pilocarpine hydrochloride can stimulate salivary gland secretions and has been shown to be effective for patients with Sjögren’s syndrome and for those who have had irradiation therapy or bone marrow transplantation. or cholinergic agent: cevimeline hydrochloride, recently was approved for use in patients with Sjögren’s syndrome. Patients using parasympathomimetic drugs, however, may experience a number of unpleasant side effects that may limit the efficacy of these medications. When conventional medical interventions do not provide satisfactory relief, or for patients with xerostomia who prefer alternative medical therapies, acupuncture may be beneficial. Patients who develop candidiasis secondary to xerostomia can be treated with oral or systemic antifungal drugs. Increasing oral moisture also may reduce the prevalence of this opportunistic infection.
A number of therapeutic interventions are available for the control and prevention of dental caries. These primarily consist of rigorous attention to personal oral hygiene, strict adherence to a non cariogenic diet, placement of sealants and the application of topical fluorides. The latter may be useful if an increased incidence of coronal caries, root caries or both becomes apparent, even when fluoridated community water is available. This strategy may be effective for both prevention of caries and possible reversal of decalcification. Supplements that contain sodium fluoride, or sodium monofluorophosphate are available for professional application as well as for home use. These products can be applied in a variety of vehicles, including gels, rinses, lozenges and chewable tablets. Interest now is focused on the use of varnishes that provide prolonged exposure to fluoride. This approach may prove to be useful for the prevention of caries associated with xerostomia.
Fluorides also are used for the management of dental caries in patients whose xerostomia has resulted from radiation therapy to the head and neck. Patients with complete dentures who experience xerostomia are more likely to develop other complications, including pain from denture irritation and loss of retention. The greater risk of developing candidiasis in edentulous patients may contribute to their discomfort. Soft denture liners orincorporation of metal in the palate of the maxillary denture have been shown to be beneficial treatment options for some patients
conclusion • Xerostomia is a condition of dry mouth that is experienced by many patients. The prevalence of this complaint and its negative effect on the patient’s quality of life make it likely that the practitioner will encounter this condition on a regular basis. Xerostomia results from the loss of saliva that may develop as a side effect from the use of medications, as a manifestation of Sjögren’s syndrome secondary to a number of connective tissue diseases or as a complication of radiation therapy. Treatment is primarily palliative, with emphasis on the use of saliva substitutes. Some patients may benefit from pharmacological stimulation of the salivary glands. The predominant complications that result from reduced saliva are dental caries, which requires comprehensive dental management and candidiasis, which can be treated with antifungal agents