Download
1 / 4
40 likes | 50 Views
Get info on Chronic Heart Failure- NICE guidance. Our chart helps to know Nice Chronic Heart Failure. This guideline covers diagnosing and managing chronic heart failure in people aged 18 and over.<br>https://www.a4medicine.co.uk/chronic-heart-failure-nice-guidance/<br>

E N D
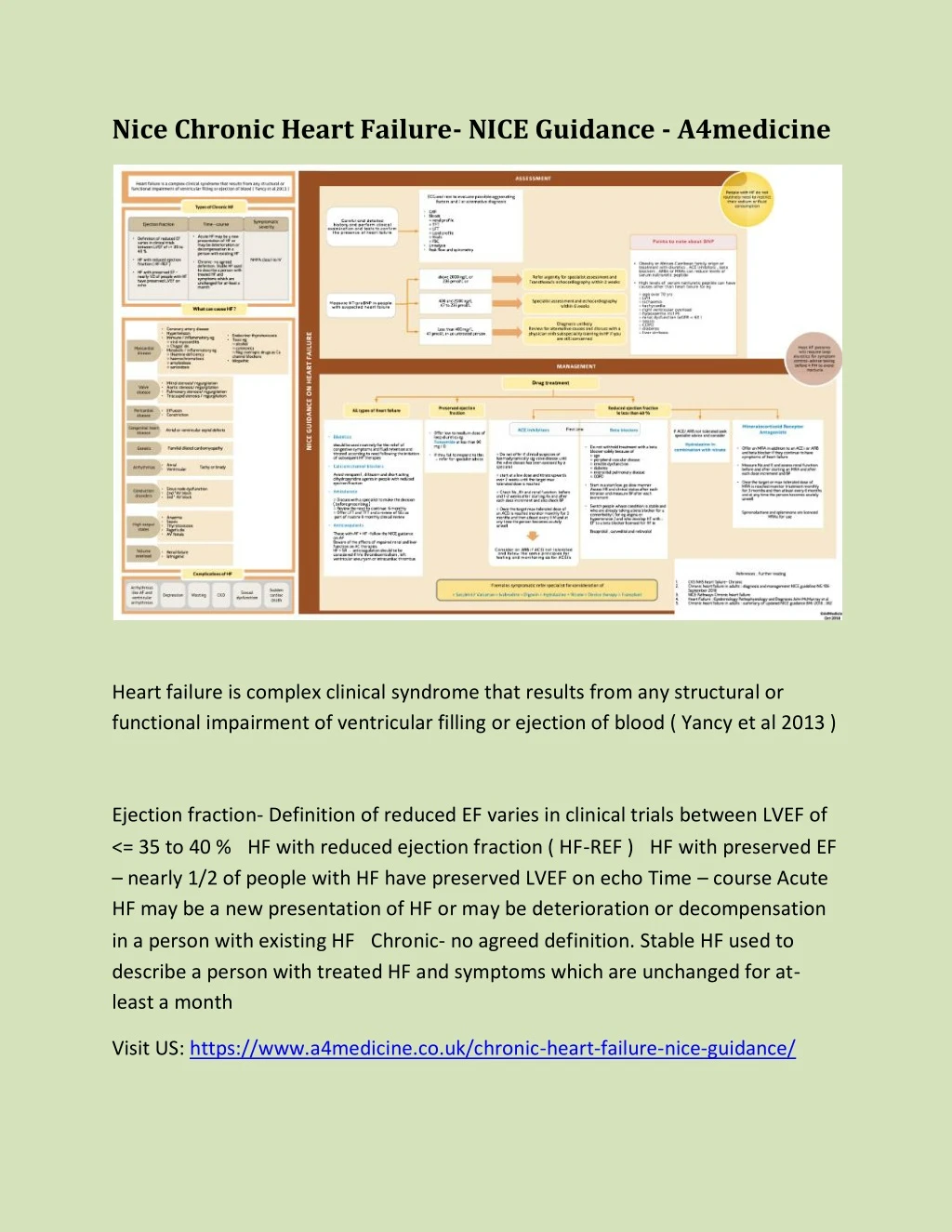
Nice Chronic Heart Failure- NICE Guidance - A4medicine Heart failure is complex clinical syndrome that results from any structural or functional impairment of ventricular filling or ejection of blood ( Yancy et al 2013 ) Ejection fraction- Definition of reduced EF varies in clinical trials between LVEF of <= 35 to 40 % HF with reduced ejection fraction ( HF-REF ) HF with preserved EF – nearly 1/2 of people with HF have preserved LVEF on echo Time – course Acute HF may be a new presentation of HF or may be deterioration or decompensation in a person with existing HF Chronic- no agreed definition. Stable HF used to describe a person with treated HF and symptoms which are unchanged for at- least a month Visit US: https://www.a4medicine.co.uk/chronic-heart-failure-nice-guidance/
Careful and detailed history and perform clinical examination and tests to confirm the presence of heart failure CXR Bloods ○ renal profile ○ TFT ○ LFT ○ Lipid profile ○ Hba1c ○ FBC Urinalysis Peak flow and spirometry ECG and rest to evaluate possible aggravating factors and / or alternative diagnosis Measure NT-proBNP in people with suspected heart failure above 2000 ng/L or 236 pmol/L or Refer urgently for specialist assessment and Transthoracic echocardiography within 2 weeks 400 and 2000 ng/L 47 to 236 pmol/L Specialist assessment and echocardiography within 6 weeks Less than 400 mg/ L 47 pmol/L in an untreated person Diagnosis unlikely Review for alternative causes and discuss with a physician with subspeciality training in HF if you are still concerned Points to note about BNPObesity or African-Carribean family origin or treatment with diuretics , ACE inhibitors , beta blockers , ARBs or MRAs can reduce levels of serum natriuretic peptide High levels of serum natriuretic peptide can have causes other than heart failure for eg ○ age over 70 yrs ○ LVH ○ ischaemia ○ tachycardia ○ right ventricular overload ○ hypoxaemia incl PE ○ renal dysfunction (eGFR < 60 ) ○ sepsis ○ COPD ○ diabetes ○ liver cirrhosis Diuretics should be used routinely for the relief of congestive symptoms and fluid retention and titrated according to need following the initiation of subsequent HF therapies Calcium channel blockers Avoid verapamil , diltiazem and short acting dihydropyridine agents in people with reduced ejection fraction Amiodarone ○ Discuss with a specialist to make the decision ( before prescribing ) ○ Review the need to continue 6 monthly ○ Offer LFT and TFT and a review of SEs as part of routine 6 monthly clinical review Anticoagulants Those with AF + HF -follow the NICE guidance on AF Beware of the affects of
impaired renal and liver function on AC therapies HF + SR → anticoagulation should be be considered if h/o thromboembolism , left ventricular aneurysm or intracardiac thrombus Offer low to medium dose of loop diuretics eg Furosemide at less than 80 mg / D If they fail to respond to this → refer for specialist advice ACE inihibitors○ Do not offer if clinical suspicion of haemodynamically sig valve disease until the valve disease has been assessed by a specialist ○ start at a low dose and titrate upwards ever 2 weeks until the target max tolerated dose is reached ○ Check Na , K+ and renal function before and 1-2 weeks after starting Rx and after each dose increment and also check BP ○ Once the target max tolerated dose of an ACEi is reached monitor monthly for 3 months and then atleast every 6 M and at any time the person becomes acutely unwell Beta blockers Do not withhold treatment with a beta blocker solely because of ○ age ○ peripheral vascular disease ○ erectile dysfunction ○ diabetes ○ interstitial pulmonary disease ○ COPD Start in a start low go slow manner Assess HR and clinical status after each titration and measure BP after each increment Switch people whose condition is stable and who are already taking a beta blocker for a comorbidity ( for eg angina or hypertension ) and who develop HF with ↓ EF to a beta blocker licensed for HF ie Bisoprolol , carvedilol and nebivolol Offer an MRA in addition to an ACE i or ARB and beta blocker if they continue to have symptoms of heart failure Measure Na and K and assess renal function before and after starting an MRA and after each dose increment and BP Once the target or max tolerated dose of MRA is reached monitor treatment monthly
for 3 months and then atleast every 6 months and at any time the person becomes acutely unwell