Download
1 / 18
180 likes | 363 Views
Moving toward universal coverage: the impact of different reform alternatives on equity in financing and utilization of health care in South Africa. JE . Ataguba D. McIntyre University of Cape Town March 15, 2011. Presentation Outline. Health Economics Unit, University of Cape Town

E N D
Moving toward universal coverage: the impact of different reform alternatives on equity in financing and utilization of health care in South Africa JE.Ataguba D. McIntyre University of Cape Town March 15, 2011
Presentation Outline Health Economics Unit, University of Cape Town South Africa Introduction Background Why this Study? Methods Findings Implications
Introduction • Inequities exist in access to heath care • The poor and those who need health care are not receiving fairer shares • Out-of-pocket payments are still high in many developing countries • Financial catastrophe and impoverishment • ‘Insurance function’ is lacking in many financing systems in Africa • Fragmentation, small risk pools, etc.
Background • Recent study in South Africa has shown that: • The distribution of health care benefits is not inline with the need for care • Health financing system is progressive • The progressivity of the financing system is attributed largely to the progressivity of private medical schemes’ contributions • Covers about 16% of the population • Mainly the richest South Africans
Background – cont’d • Universal health systems is now being promoted to replace fragmented financing options and improve access to health care • Not just about financing but the whole system • South African gov’t recently announced commitment to this • The Polokwane conference (2007) • No official document about this is out yet • There are some concerns about the long-run feasibility and sustainability of the proposed system
Why the study? • Need scientific evidence to provide further insights into the equity implications of the proposed reforms • Will the reforms improve the distribution of health care benefits? • What about the distribution of financing burden? • We attempt to examine the long-run (over a 15 year period) equity implications of the proposed health system reforms
Methods • The precise nature of the reforms has not been finalised • The proposed reforms are currently contested by some stakeholders • However we simulated three detailed possible alternative scenarios (based on interviews with key health sector actors) • Status quo (SQ) • Social health insurance (SHI) • Universal coverage (UC)
Methods • Status quo • Leaving the current system largely unchanged • The richer groups being covered by private insurance • the rest by tax-funded health services • SHI • Extending private health insurance coverage to more formal sector workers about tax-threshold • Continuing to fund health services for others from general tax revenue • Universal coverage • Comprehensive package of services for all citizens • Funded by allocations from general tax revenue, and • Mandatory payroll health tax
Methods • Benefit incidence analysis • Distribution of total public benefits • Distribution of total private benefits • Distribution of total (public and private) benefits • Utilization norms developed for primary and hospital care services (Monitor Company et al., 1996; Rispel et al., 1996) • Used to project future utilization rates • Controlling for the HIV/AIDS burden
Methods • The utilisation rates and real unit costs at the end of the 15-year period were used • For those covered by private schemes and those not covered by private medical schemes • Benefits = Utilization * unit cost • Data from a 2008 HH survey • Use of health services • Distribution of financing burden • Work in progress!!!
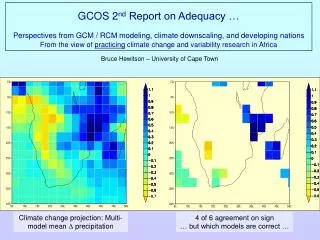
Distribution of total (public + private) health care benefits .
Major findings • Private health care benefits • The status quo model shows a less pro-rich distribution than the SHI or UC • UC is the most pro-rich. • Because only the rich will belong to private medical schemes and use mainly private services • Public health care benefits • The SHI model shows a more pro-poor distribution • Note that the very poor are not covered under the medical schemes more pressure on the public sector services • The UC model is less pro-poor • Note that both the rich and the poor now use the public system
Major findings • Total health care benefits • The UC model is almost proportional • Both the rich and the poor obtain fair shares of benefits • Here, the bottom 40% of the population are receiving about 40% of total health care benefits • The SQ and the SHI models show clearly pro-rich distributions • They are less ‘equitable’ than the UC option
Implications • The UC model shows some slight pro-rich distribution (though not statistically significant) • The very rich who can afford private insurance cover will still choose expensive private care • The Universal Coverage model in total produces a more equitable distribution of health care benefits in the long-run compared to the SQ and SHI models.