Download
1 / 26
290 likes | 1.22k Views
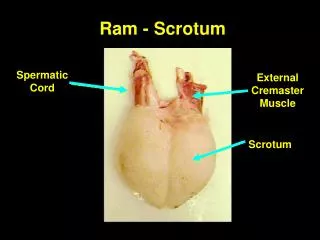
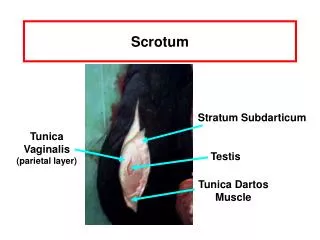
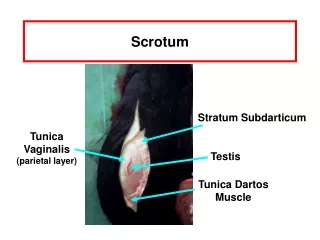
Acute SCROTUM. Testicular torsion Appendage torsion Epidydimitis Orchitis Trauma Tumor ? Hernia ?. Testicular Anatomy. The normal testis is oriented in the vertical axis and the epididymis is above the superior pole in the posterolateral position.

E N D
Acute SCROTUM • Testicular torsion • Appendage torsion • Epidydimitis • Orchitis • Trauma • Tumor ? • Hernia ?
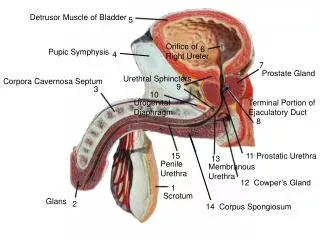
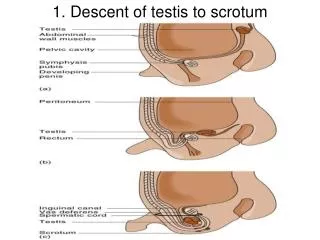
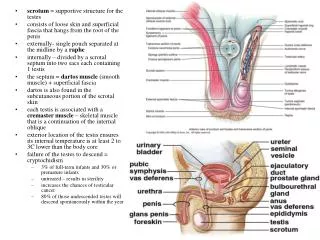
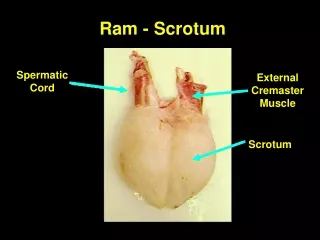
Testicular Anatomy • The normal testis is oriented in the vertical axis and the epididymis is above the superior pole in the posterolateral position. • Cremasteric reflex: Stroking/pinching the inner thigh should result in elevation of > 0.5 cm of the ipsilateral testicle
Testicular Torsion • Incidence 1:4000 • Only 50% salvageability w/ testicular loss from either atrophy or ochiectomy • Two peak periods: first year of life and at puberty • 10 times more likely in an undescended testis
Testicular Torsion Most torsions due to bilateral anatomic abnormality. Tunica vaginalis has a high insertion about the spermatic cord. Resultant bell-clapper deformity—testis dangles in the scrotum and is mobile
Testicular Torsion: Pathophysiology • Initially venous return is obstructed and then venous thrombosis is followed by arterial thrombosis • Degree of obstruction is a function of the degree of rotation • Necrosis develops in testicle with complete obstruction and infarction develops after arterial thrombosis
Testicular Torsion • Rapid swelling and edema of the testis and scrotum, followed by scrotal erythema • Damage proportional to duration/extent of vascular obstruction • Salvage rate of testis is 80-100% if pain lasts less than 6 hours • Pain > 24 hours is associated w/ testicular infarction
Testicular Torsion • 40% report a hx of similar pain that resolved spontaneously in the past • Often occurs after exertion or during sleep • Typically no urinary symptoms • Sudden onset of scrotal pain, but can be inguinal or lower abdominal. May be constant or intermittent. Not positional • Nausea and Vomiting
Testicular Torsion • Hemiscrotum is swollen, tender, firm • High-riding testis with a transverse lie is classic sign • Loss of cremasteric reflex – almost universal • May see the bell-clapper deformity, with horizontal lie of the contralateral testicle • Prehn’s sign: Relief of scrotal pain by elevating testicle. NOT a reliable way to distinguish epididymitis from torsion
Testicular Torsion: Diagnosis • Doppler Ultrasononography now test of choice for Dx of torsion. Sensitivity comparable to radioisotope scans (86%-100%) and greater specificity (100%). Doppler U/S is more rapid and more available than radioisotope scans.
Testicular Torsion: Management • Immediate Urologic consultation for surgical exploration and possible bilateral orchidopexy if diagnosis is obvious • Manual detorsion - Only a temporizing measure. Endpoint for successful detorsion is pain relief. • Most torsions occur lateral to medial, therefore detorsion should be attempted in a medial to lateral direction - “open the book” maneuver • Imaging if diagnosis unclear, should NOT delay exploration if high suspicion exists
Torsion of Appendage • Torsion of appendages is more common than testicular torsion • Testicular and Epididymal appendages are vestigial remnants of the wolffian and mullerian ducts respectively • Most frequent in preadolescent males 3-13, appendix testis > epididymal appendix • Cause unclear • Twisting causes obstruction, edema and then painful necrosis
Torsion of Appendage • Discrete, painful testicular mass • Symptoms less severe than torsion. No nausea, vomiting, or fevers • Transillumination of scrotum may reveal the cyanotic appendage as a pathognomonic blue dot • U/S or Nuclear scintigraphy should reveal normal to increased blood flow
Torsion of Appendage: Management • Scrotal Support • Pelvic rest • Analgesia • Expect resolution of symptoms in 7-10 days with degeneration of appendages
Epididymitis • Average age 25 years • Most common misdiagnosis for testicular torsion • Rarely affects a prepubertal child without an underlying urinary tract infection • Result of retrograde ascent of urethral and bladder pathogens • Peritubular fibrosis may develop and occlude the ductules, if bilateral may lead to sterility
Epididymitis In men > 40, E. coli is the predominant pathogen. Other coliform organisms, Pseudomonas, and gram positive cocci. Associated w/ underlying urologic pathology -- Recent GU tract manipulation or bacterial prostatitis. In men <40, Chlamydia and N. gonorrhoeae are the major pathogens
Epididymitis • Gradual Scrotal pain, peaks over days • Low grade fever, average 38 degrees C • Cremasteric reflex usually preserved • Due to inflammatory nature of pain, may have some transient pain relief from scrotal elevation • Localized epididymal swelling initially, then may progress to single, large testicular mass • Urethral discharge and voiding symptoms may be present
Epididymitis • Pyuria and bacteriuria on U/A • Urethral discharge should be examined for gram stain and culture • Leukocytosis between 10K-30K • Torsion should not be excluded by pyuria, fever, or dysuria. An equivocal exam demands Imaging. U/S with increased or normal testicular blood flow is c/w epididymitis
Epididymitis: Management • Sexually acquired: Ceftriaxone 250 mg IM and Doxycycline 100 mg PO bid x 10d. Treat sexual partners. • Nonsexually acquired: TMP-SMX or Fluoroquinolone x 14d. Check urine C&S. • Bed rest, scrotal support, analgesics, sitz baths, and Urology follow up
Complications of Epididymitis • Infertility - Sexually transmitted epididymitis • Abscess - Gonococcal epididymitis • Chronic epididymitis • U/S indicated if no response to medical therapy
Orchitis • Acute infection of the testis • Rare without initial epididymitis. Consider testicular tumor. • Bacterial infection secondary to spread from epididymitis of E. coli, Klebsiella, Pseudomonas • Viral orchitis – Mumps. 4-6 days after onset of parotitis usually. 50% of involved testes atrophy but infertility rare • Syphilis • Treatment: Antibiotics for bacterial orchitis and local scrotal measures for viral orchitis
Testicular Tumor • Testicular CA – Most common cause of malignancy to afflict young men • Average age of incidence 32 • DDx: Epididymitis and torsion • Increased incidence with cryptorchidism in bilateral testes • Majority are Seminomas, then embryonal cell CA and teratomas
Testicular Tumor • Classic presentation – Painless, firm testicular mass • Acute hemorrhage within the tumor can lead to acute scrotal pain (10%) • Ultrasound – Distinct Intratesticular Mass • CXR if suspect Metastases • Treatment: Immediate Urology referral. Radical orchiectomy. Cisplatin chemotherapy and Radiation for seminomas.