Download
1 / 40
400 likes | 811 Views
The Case of the Painful Leg . David Mansoor Radiology, Feb 2004. HPI. 12 y.o. male with 1 year history left thigh pain Acute onset 1 year ago and has persisted since No inciting event “pressure” sensation on inner part of left thigh Denies sharp or shooting sensations

E N D
The Case of the Painful Leg David Mansoor Radiology, Feb 2004
HPI • 12 y.o. male with 1 year history left thigh pain • Acute onset 1 year ago and has persisted since • No inciting event • “pressure” sensation on inner part of left thigh • Denies sharp or shooting sensations • Denies numbness or weakness • Increases in severity with activity • Predominately at night, makes it hard to sleep • Denies constitutional sxs (fevers, weight loss, etc)
None Aspirin 225mg bid Left proximal medial thigh tenderness No limitations in ROM No pain with movement Normal gait PMH PE
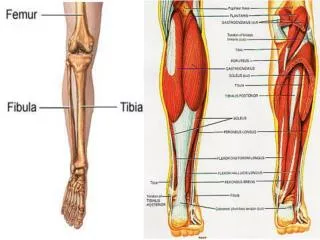
Idiopathic (growing pain) Trauma (muscle bruise, fracture, etc) Bone tumor (malignant—osteosarcoma, Ewing’s tumor; benign—osteoblastoma, osteoid osteoma; metastatic) Infection and inflammation (osteomylitis, myositis, TB, etc) Other (slipped capital femoral epiphysis, Legg Calve Perthe’s Dz, etc) DDx of Leg Pain in Children
CBC Electrolytes X-Ray ABG More history CT Workup (you choose)…
Diagnosis… • Osteoid Osteoma • A benign skeletal neoplasm of unknown etiology, usually smaller than 1.5cm • Consists of a central small nidus of osteoid surrounded by a zone of reactive sclerotic bone • (osteoid is immature bone that has not yet undergone calcification)
Histology • Nidus of osteoblasts and osteoid arranged in a haphazard fashion • Sharp demarcation between nidus and reactive bone • The nidus is highly vascular
Epidemiology • Accounts for 10% of all benign bone tumors • Males are effected twice as much as females • Age range 5-56 • 90% are 5-25 • Proximal femur>tibia>spine>humerus
No malignant potential Occasionally regresses spontaneously May induce scoliosis if spinal column is involved Pain, pain, pain Skeletal bone pain Worsens at night Worsens with EtOH Relieved by aspirin Mortality/Morbidity
Radiography CT MRI Bone Scan U/S Angiography Imaging Modalities
Radiography • Can provide the best diagnostic capacity when coupled with clinical history • Ovoid lucent defect seen in 75% • Some areas are difficult to assess • Spine (but look for scoliosis), femoral neck, small bones of hands and feet, intraarticular (but look for joint effusion) • New bone formation can mask nidus • Osteomyelitis mimics
CT • Ultimate diagnosis for precise localization of nidus and guiding percutaneous ablation • Great for areas with complex anatomy such as spine and femoral neck
MRI • Nidus is usually masked by sclerotic bone • Presence of marrow and soft tissue edema closely simulate osteomyelitis on MRI • Good for intraarticular lesions, as the osteoma causes synovial thickening, inflammation, and joint effusion • Not usually utilized
Bone Scan • Technetium-99 bone scan shows area of increased uptake • Very sensitive technique • Findings may be positive before radiographic changes are present • Specificity is low
U/S • Limited studies to date • Duplex color Doppler U/S demonstrates the highly vascular nidus • Can help dx intra-articular osteoid osteomas, but not well studied • Cortical irregularity and focal synovitis
Angiography • Useful because the osteoid osteoma is highly vascular • Characteristic blush seen in venous phase • May be useful in differentiating tumor from osteomyelitis • Invasive so rarely used
Treatment • Removal of the nidus is the only way to cure • Surgical (invasive, not usually used) • Ablation is the mainstay of treatment • Percutaneous • Radiofrequency* • Ethanol • Laser • Thermocoagulation
First report of success by Rosenthal et al. in 1992 Now considered to be safe, minimally invasive, and cost-effective treatment Radiologists role is not only to diagnose but also treat!! Training is offered to musculoskeletal & interventional fellows Radiofrequency Thermal Ablation: CT Guided Rosenthal D, Rosenberg A, Springfield D. Ablation of Osteoid Osteomas with a Percutaneously Placed Electrode: A New Procedure. Radiology. 1992; 183:29-33
RTA: Principle • Alternating current of high-frequency radio waves passes from the electrode tip in body tissue and dissipates its energy as heat • Different than electrocautery in that the tissue around the electrode (rather than the electrode itself) is the primary source of heat
RTA cont’d • Should only be performed when definite nidus is visualized • CT guided affords best visualization of needle and probe placement directly within nidus • General anesthesia is used as entering the nidus is VERY painful; also to prevent patient movement
Contraindicated in patients with cardiac pacemakers Complications during needle passage: bleeding and nerve injury Complications also include soft-tissue burns, infection, skin necrosis in superficially located tumors RTA: Contraindications and Complications
RTA: Technique • Determine precise location of lesion using CT • Plan an entry point perpendicular to the skin surface; aim is to puncture in the scan plane • Insert penetration cannula (confirm position with serial scans) • Insert drill through cannula and drill to the edge of nidus (confirm location with further scans) • Remove drill and insert RF probe
RTA: Technique cont’d • Temperature at end of probe is 90 C, kept there for 4 minutes • 50% of ptnts will have a physiological reaction (increased HR, BP, etc)
RTA: Postprocedure Healing • Pain afterwards is variable • Up to 1 or 2 days after the procedure • Analgesia is rarely required • Can bear weight immediately after and return to normal activities • Resolution of pain is used to define successful treatment • Success rate of 92% in 130 patients Pinto et al. Technical Considerations in CT-guided Radiofrequency Thermal Ablation of Osteoid Osteoma: Tricks of the Trade. American Journal of Radiology. December 2002.
Growing Pains • Common in kids age 5-10 • Not very well localized, worse at night • Not chronic • Should not keep kids up at night • Radiographic findings: normal
Trauma • Not likely as there is no inciting event • However…stress fractures don’t have a clear inciting event • tibial stress fractures are most common in children, then metatarsal stress fractures • femoral stress fractures are rare and usually found in endurance athletes • Radiography: fracture may not appear for 2-10 weeks after symptom onset; MRI & bone scintigraphy more sensitive
Tumor • Likely, given persistence as well as focal location of symptoms • Radiography: vary greatly
Infection • Can be chronic osteomyelitis (despite lack of fever) • Radiography: areas of ill defined bone destruction with cortical thickening (causes sclerosis and widening of bone)
Slipped capital femoral epiphysis Most common hip disorder in teens, occurs during growth spurt boys>girls, usually overweight Fracture through growth plate of proximal femur with relative slip of the epiphysis (femoral head “slips” off neck of femur)* Persistent pain with limp radiography Legg Calve Perthe’s Disease Idiopathic avascular necrosis of the femoral head Most common in boys 4-10 Persistent pain with limp, limited range of motion, atrophy of upper thigh muscles radiography Other
SCFE • Widened physeal plate • Metaphysis displaced laterally
LCPD • Femoral head appears mottled • Femoral neck is shortened and thickened • Acetabulum is flattened
More History • Pain is relieved by aspirin but not tylenol or ibuprofen
CBC • normal
Electrolytes • Normal
ABG • Normal
Radiography • At base of femoral neck medially is a small lucent area surrounded by more dense bone • Nidus usually smaller than 1.5cm
CT • Notice the radioluscent central nidus surrounded by the thickened cortex