Download
1 / 36
360 likes | 1.08k Views
Monitoring performance and governance including maternity ‘dashboard’. Helen Scholefield Clinical Director Obstetrics Liverpool Women’s NHS Foundation Trust Edwin Chandraharan Lead Clinician Labour Ward & Clinical Governance in Obstetrics & Gynaecology St. George’s Healthcare NHS Trust.

E N D
Monitoring performance and governance including maternity ‘dashboard’ Helen Scholefield Clinical Director Obstetrics Liverpool Women’s NHS Foundation Trust Edwin Chandraharan Lead Clinician Labour Ward & Clinical Governance in Obstetrics & Gynaecology St. George’s Healthcare NHS Trust
League Tables • Organisational performance • Annual Health Check • Health Care Commission Survey • CNST / NHSLA • Dr Foster • FT Benchmarking • CEMACH Perinatal Mortality figures • Individual performance in obstetrics • Cf cardiac surgeons
Clinical Governance in Practice: Experience with ‘Maternity Performance and Governance Score Card’ Edwin Chandraharan Lead Clinician Labour Ward & Lead for Clinical Governance in Obstetrics & Gynaecology St. George’s Healthcare NHS Trust
Background Hypoxic-Ischaemic- Encephalopathy (HIE): - ‘Birth Asphyxia’ - Short term & long term sequelae • 6 cases / 2005 at St. George’s ??Excessive - External Review Panel (‘ HIE Panel’)
Areas identified by the ‘HIE Panel’ for action • Communication and Team Working • STAN Training • Staffing: recruitment & retention • Risk Management Process • Education and Training
Clinical Governance • ‘Framework through which the NHS Organisations are responsible for safeguarding good clinical practice and continuously improving patient care by creating an environment, where clinical excellence would flourish’ • How do we assess and monitor the strategies for clinical governance on the ground in maternity services? • How to we effect changes in day-to-day practice? Performance & Governance Score Card
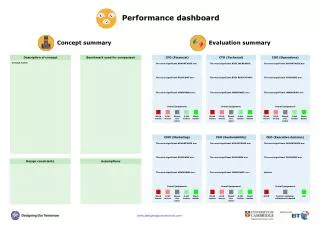
St. George’s Experience with Performance & Governance Score Card ‘Maternity Dashboard’ • Designed by Prof. Arulkumaran & Team –Northwick Park • Recommended by CMO’s Report • Looks at Activity, Staffing, Clinical Risk indicators, User feedback (e.g. complaints)
Can Robust and Effective Monitoring through the Maternity Dashboard help improve Quality of Patient Care?
Example of an Obstetric assurance presentation to Board Helen Scholefield Clinical Director, Obstetrics Liverpool Women’s NHS Foundation Trust
Obstetric Risk Management Strategy • Annual update August 07- Needs ratifying by CGC • Will be monitored through the Maternity Risk Management Group. • Associated reports and action plans will be monitored by the Risk Management Committee. • Risk related reports from the Directorate will be further monitored by the appropriate senior committee in the Trust. • Staff will be informed of the principles of this strategy and all associated policies at local induction, annual training and workshops • Adherence to the principles of the strategy will be monitored through associated reports, action plans, changes in practice and the PDR process
Stillbirth 2004 Neonatal Mortality Perinatal Mortality 2005 2004
Comparison with other units with similar referral patterns (2004) Stillbirth rates for Liverpool Women's Hospital NHS Foundation Trust (LWH), although higher than the National rate of 5.7/1000, are similar to other tertiary referral centres.
Stillbirth rate corrected for women who originally booked and delivered at LWH
Themes • Themes: • The major themes identified for were: • Undetected intrauterine growth restriction/small for gestational age babies • Late bookers, unbooked women and women who did not attend antenatal visits • Late transfers for antenatal care from other areas • CTG misinterpretation • Other issues identified were: • Failure of staff to recognise relevance of past obstetric history or complexity of current pregnancy • Fetal assessment in large women
Conclusions • How do we improve the detection of the small for gestational age fetus at risk of stillbirth? • How we improve the stillbirth rate for obese women? • How do we improve antenatal CTG interpretation within the context of the complexity of the case? • How do we improve our services for vulnerable women, women who book late or transfer care late in pregnancy? • We need to look at the relationship between obstetric practice and high neonatal death rate
Changes in Practice and their impact • Profile and communication relating to anaesthetic cover for 24 hour – Improved epidural provision • Improved relations & communication between intrapartum areas and deployment of staff, - reduction in number of delayed IOL • Meditech facility relating to PCI identification & subsequent care plans for vulnerable women and babies utilised - No further ACE’s • Booking assessment sheet sent to CMW, reducing risks of DNA – fewer incidents • Anti D policy change in procedure- No further ACE’s • Formal record of identification at birth by 2 individuals - reduction in number of babies identified incorrectly following • Transfer of management of TC to NICU - Admission and transfer improved • Medication errors decreased following individual feedback • TTO storage/ prep area identified -No further ACE’s • Training of clerical staff - Improvement in patient record incidents and reduction in record unavailability • Training on CD procedures and separate CD record book for theatre - No further reports of non- compliance
Risk Register • 60 on register • High risks – none • Medium and low risk where significant e.g. trends • Medication Errors –Medicines Management Working party • Patient Records – Out of hours access to Aintree notes • Lone worker system • Poor ergonomics • Obstetric Secretaries • Specialist MW
RR- Changes in practice (controls) and impact of changes • Discharge arrangements • Emergency call system on Jeffcoate/ MLU • Sinks replaced on Postnatal wards • Improved liaison and formal handover between Intrapartum areas • Improved provision of epidural - reduced number of patient complaints and incidents reported • Identified process for robust patient information review • All Obstetric Guidelines now accessible via Trust intranet • Development of Obstetric Risk Management Newsletter
Complaints Themes Staff Attitude Lack of support on PN ward Assessment room Wrong documentation
Clinical Audit Audit programme on target to meet CNST & NHSLA requirements
Guidelines Compliant with: Antenatal Care CS AN & PN Mental Health PN Care IPG Compliant with Amnioinfusion Pleuro- amniotic shunt Bladder shunt Cell salvage Other procedures with IPG not done NICE Guidance
NSF The Action plan has been reviewed regularly and updated and is now complete and the Directorate declared compliance with recommendations
Confidential Enquiries • Project 27/28. Joint action plan led by Neonatal Directorate developed in response toCESDI recommendations Action plan completed. • CEMACH . Action plan developed in Response to National Confidential Enquiry into Maternal and Child Health 2004 (2000-2002) Compliant • Non-compliance: • Awaiting Action plan for CEMACH Diabetes Survey
HCC Northwick Park Reports • Action plan in place • Areas of partial compliance • Consultant Staffing • Hours of DS cover • Dedicated cover for CS lists • MW staffing shortage on DS • 24 Hour theatre cover • Interventional radiology
Infection Control • Concerns re compliance due to impact of key staff leaving. • Ward managers have been informed of where action plans are out of date and audits have not taken place. • They arranging these and liaising with their link midwives • Trial of use of PDA for area audits to improve timely feedback • Will utilize Theatres & CC spread sheet which identifies when audits are due with hyper links into Winning Ways and Saving Lives when these assessments are also due • Action to take place: • Complete audits • Develop action plans for any lack of improvement in practice identified, with additional controls put in place where neded.
CNST Maternity 76% of Midwifery staff completed obstetric emergency training Expect to reach 90% target by Jan 08 Junior medical staff completed as part of induction Consultants currently updating. No figures received from PG NHSLA General Compliant: Infection Control, Risk Management & Incident Reporting, Health & Safety training, Manual Handling, Blood Transfusion and Basic Life Support, corporate/ local induction. Partial compliance: Conflict resolution Being Open Protecting Vulnerable adults Safe Guarding Children Training
NHSLA General Standards & CNST Maternity Standards All non- compliance noted in NHSLA and CNST action plans with identified individual responsibility and time frame for submission. Anticipate compliance at level 3 Standards for Better Health All non- compliance noted in Standards for Better Health action plan with identified individual responsibility and time frame for submission. (see Risk Management Assurance Report- circulated)