Download

1 / 26
300 likes | 1.16k Views
Antifungal Agents. Lindsay Mayer, PharmD October 26, 2007. MOA: Binds to ergosterol within the fungal cell membrane resulting in depolarization of the membrane and the formation of pores. The pores permit leakage of intracellular contents. Exhibits concentration dependent killing.

E N D
Antifungal Agents Lindsay Mayer, PharmD October 26, 2007
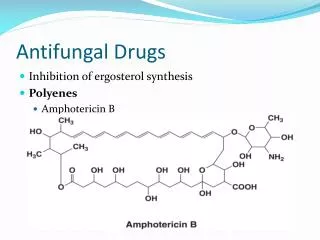
MOA: Binds to ergosterol within the fungal cell membrane resulting in depolarization of the membrane and the formation of pores. The pores permit leakage of intracellular contents. Exhibits concentration dependent killing. Polyenes—Amphotericin B
Polyenes—Amphotericin B • Spectrum of Activity • Broad spectrum antifungal • Active against most molds and yeasts • Holes: C. lusitanae, Fusarium, Tricosporon, Scedosporium
Polyenes—Amphotericin B • Resistance • Susceptibility testing methods have not been standardized • Development of resistance in a previously susceptible species is uncommon • Mechanisms of Resistance • Reductions in ergosterol biosynthesis • Synthesis of alternative sterols that lessen the ability of amphotericin B to interact with the fungal membrane
Polyenes—Amphotericin B • Isolated from Streptococcus nodosus in 1955 • Amphotericin B is “amphoteric” • Soluble in both basic and acidic environments • Insoluble in water Formulations • Amphotericin B deoxycholate • Fungizone • Amphotericin B colloidal dispersion • Amphotec, Amphocil • Amphotericin B lipid complex • Abelect • Liposomal amphotericin B • Ambisome
Amphotericin B deoxycholate • Distributes quickly out of blood and into liver and other organs and slowly re-enters circulation • Long terminal-phase half-life (15 days) • Penetrates poorly into CNS, saliva, bronchial secretions, pancreas, muscle, and bone • Disadvantages • Glomerular Nephrotoxicity—Dose-dependent decrease in GFR because of vasoconstrictive effect on afferent renal arterioles • Permanent loss of renal function is related to the total cumulative dose • Tubular Nephrotoxicity—K, Mg+, and bicarbonate wasting • Decreased erythropoietin production • Acute Reactions—chills, fevers, tachypnea • Support • Fluids • Potassium replacement • Avoid concurrent nephrotoxic agents • Premed with acetaminophen, diphenhydramine or hydrocortisone • Meperidine for rigors • Dose: 0.3 to 1 mg/kg once daily
Amphotericin B Colloidal Dispersion(Amphotec) • Cholesterol sulfate in equimolar amounts to amphotericin B • Similar kinetics to amphotericin B deoxycholate • Acute infusion related reactions similar to amphotericin B deoxycholate • Reduced rates of nephrotoxicity compared to amphotericin B deoxycholate • Dose • 3 to 4 mg/kg once daily
Amphotericin B Lipid Complex(Abelcet) • Equimolar concentrations of amphotericin and lipid • Distributed into tissues more rapidly than amphotericin B deoxycholate • Lower Cmax and smaller AUC than amphotericin deoxycholate • Highest levels achieved in spleen, liver, and lungs • Delivers drug into the lung more rapidly than Ambisome • Lowest levels in lymph nodes, kidneys, heart, and brain • Reduced frequency and severity of infusion related reactions • Reduced rate of nephrotoxicity • Dose • 5 mg/kg once daily
Liposomal Amphotericin B (AmBisome) • Liposomal product • One molecule of amphotericin B per 9 molecules of lipid • Distribution • Higher Cmax and larger AUC • Higher concentrations achieved in liver, lung, and spleen • Lower concentrations in kidneys, brain, lymph nodes and heart • May achieve higher brain concentrations compared to other amphotericin B formulations • Reduced frequency and severity of infusion related reactions • Reduced rate of nephrotoxicity • Dose • 3 to 6 mg/kg once daily
Flucytosine • MOA • Converted by cytosine deaminase into 5-fluorouracil which is then converted through a series of steps to 5-fluorouridine triphosphate and incorporated into fungal RNA leading to miscoding • Also converted by a series of steps to 5-fluorodeoxyuridine monophosphate which is a noncompetitive inhibitor of thymidylate synthase, interfering with DNA synthesis Fluorinated pyrimidine
Flucytosine • Spectrum of Activity • Active against • Candida species except C. krusei • Cryptococcus neoformans • Aspergillus species • Synergy with amphotericin B has been demonstrated • The altered permeability of the fungal cell membrane produced by amphotericin allows enhanced uptake of flucytosine • Mechanisms of Resistance • Loss of cytosine permease that permits flucytosine to cross the fungal cell membrane • Loss of any of the enzymes required to produce the active forms that interfere with DNA synthesis Resistance occurs frequently and rapidly when flucytosine is given as monotherapy Combination therapy is necessary
Flucytosine • Half-life • 2 to 5 hours in normal renal function • 85 hours in patients with anuria • Distributes into tissues, CSF, and body fluids • Toxicities • Bone marrow suppression (dose dependent) • Hepatotoxicity (dose dependent) • Enterocolitis Toxicities occur more commonly in patients with renal impairment • Dose • Administered orally (available in 250 and 500 mg capsules) • 100 to 150 mg/kg/day in 4 divided doses • Dose adjust for creatinine clearance • Flucytosine concentrations should be monitored especially in patients with changing renal function • Contraindicated in pregnancy
Triazoles • MOA: Inhibits 14-α-sterol demethylase, which is a microsomal CYP450 enzyme. This enzyme is responsible for conversion of lanosterol to ergosterol, the major sterol of most fungal cell membranes
Triazoles—Fluconazole • Dose • 100 to 400 mg daily • Renal impairment: • CrCl >50 ml/min, give full dose • CrCl<50 ml/min, give 50% of dose • Dialysis: replace full dose after each session • Drug Interactions • Minor inhibitor of CYP 3A4 • Moderate inhibitor of CYP 2C9 • Warfarin, phenytoin, cyclosporine, tacrolimus, rifampin/rifabutin, sulfonylureas • Adverse Drug Reactions • Well tolerated • Nausea • Elevated LFTs UNC Hospital Formulary
Triazoles—Itraconazole • Dose • 200 to 400 mg/day (capsules) • doses exceeding 200 mg/day are given in 2 divided doses • Loading dose: 200 mg 3 times daily can be given for the first 3 days • Oral solution is 60% more bioavailable than the capsules • Drug Interactions • Major substrate of CYP 3A4 • Strong inhibitor of CYP 3A4 • Many Drug Interactions • Adverse Drug Reactions • Contraindicated in patients with CHF due to negative inotropic effects • QT prolongation, torsades de pointes, ventricular tachycardia, cardiac arrest in the setting of drug interactions • Hepatotoxicity • Rash • Hypokalemia • Nausea and vomiting
Triazoles—Voriconazole • Dose • IV • 6 mg/kg IV for 2 doses, then 3 to 4 mg/kg IV every 12 hours • PO • > 40 kg—200-300 mg PO every 12 hours • < 40 kg—100-150 mg PO every 12 hours • Cirrhosis: • IV • 6 mg /kg IV for 2 doses, then 2 mg/kg IV every 12 hours • PO • > 40 kg—100 mg PO every 12 hours • < 40 kg— 50 mg PO every 12 hours • Renal impairment: • if CrCl<50 ml/min, use oral formulation to avoid accumulation of cyclodextrin solubilizer
Common Adverse Effects Peripheral edema Rash (6%) N/V/D Hepatotoxicity Headache Visual disturbance (30%) Fever Serious Adverse Events Stevens-Johnson Syndrome Liver failure Anaphylaxis Renal failure QTc prolongation Triazoles—Voriconazole • Drug Interactions • Major substrate of CYP 2CD and 2C19 • Minor substrate of CYP 3A4 • Weak inhibitor of CYP 2C9 and 2C19 • Moderate inhibitor of CYP 3A4 • Dose Adjustments • Efavirenz • Phenytoin • Cyclosporine • Warfarin • Tacrolimus
Triazoles—Posaconazole • Dosing (only available PO) • Prophylaxis of invasive Aspergillus and Candida species • 200 mg 3 times/day • Treatment of oropharyngeal candidiasis • 100 mg twice daily for 1 day, then 100 mg once daily for 13 days • Treatment or refractory oropharyngeal candidiasis • 400 mg twice daily • Treatment of refractory invasive fungal infections (unlabeled use) • 800 mg/day in divided doses • Drug Interactions • Moderate inhibitor of CYP3A4 • Adverse Reactions • Hepatotoxicity • QTc prolongation • GI: Diarrhea
Echinocandins MOA Irreversibly inhibits B-1,3 –D glucan synthase, the enzyme complex that forms glucan polymers in the fungal cell wall. Glucan polymers are responsible for providing rigidity to the cell wall. Disruption of B-1,3-D glucan synthesis leads to reduced cell wall integrity, cell rupture, and cell death.
Echinocandins—Spectrum of Activity Gallagher JC, et al. Expert Rev Anti-Infect Ther 2004;2:253-268
Echinocandin—Drug Interactions • Caspofungin • Not an inducer or inhibitor of CYP enzymes • CYP inducers (i.e. phenytoin, rifampin, carbamazepine) • Reduced caspofungin levels • Increase caspofungin dose • Cyclosporine • Increases AUC of caspofungin • Hepatotoxicity • Avoid or monitor LFTs • Tacrolimus • Reduced tacrolimus levels by 20% • Monitor levels of tacrolimus • Micafungin • Minor substrate and weak inhibitor of CYP3A4 • Nifedipine • Increased AUC (18%) and Cmax (42%) of nifedipine • Sirolimus • Increased concentration of sirolimus • Anidulafungin • No clinically significant interactions Cappelletty et al. Pharmacotherapy 2007;27:369-88
Echinocandins—Adverse Effects • Generally well tolerated • Phlebitis, GI side effects, Hypokalemia • Abnormal liver function tests • Caspofungin • Tends to have higher frequency of liver related laboratory abnormalities • Higher frequency of infusion related pain and phlebitis
References • Gallagher JC, et al. Expert Rev Anti-Infect Ther 2004;2:253-268 • UNC Hospital Formulary • Patel R. Antifungal Agents. Part I. Amphotericin B Preparations and Flucytosine. Mayo Clin Proc 1998;73:1205-1225 • Terrel CL. Antifungal Agents. Part II. The Azoles. Mayo Clin Proc 1999;74:78-100. • Mehta J. Do variations in molecular structure affect the clinical efficacy and safety of lipid based amphotericin B preparations? Leuk Res. 1997;21:183-188. • Groll AH et al. Penetration of lipid formulations of amphotericin B into cerebral fluid and brain tissue. 37th ICAAC, 1997. Abstract A90. • Gallagher JC et al. Recent advances in antifungal pharmacotherapy for invasive fungal infections. Expert Rev. Anti-infect. Ther 2004; 2: 253-268. • Groll AH et al. Antifungal Agents: In vitro susceptibility testing, pharmacodynamics, and prospects for combination therapy. Eur J Clin Microbiol Infect Dis 2004;23:256-270. • Capelletty D et al. The echinocandins. Pharmacotherapy 2007;27:369-388. • Spanakis EK et al. New agents for the treatment of fungal infections: clinical efficacy and gaps in coverage. Clin Infect Dis 2006;43:1060-8. • Rex JH, Stevens DA. Systemic Antifungal Agents. In: Mandell GL, Bennet JE, Dolin R, eds. Mandell, Douglas, and Bennett’s: Principles and Practice of Infectious Diseases. Vol 1. 6th ed. New York, NY: McGraw-Hill;2005:502.