Download
1 / 22
220 likes | 1.1k Views
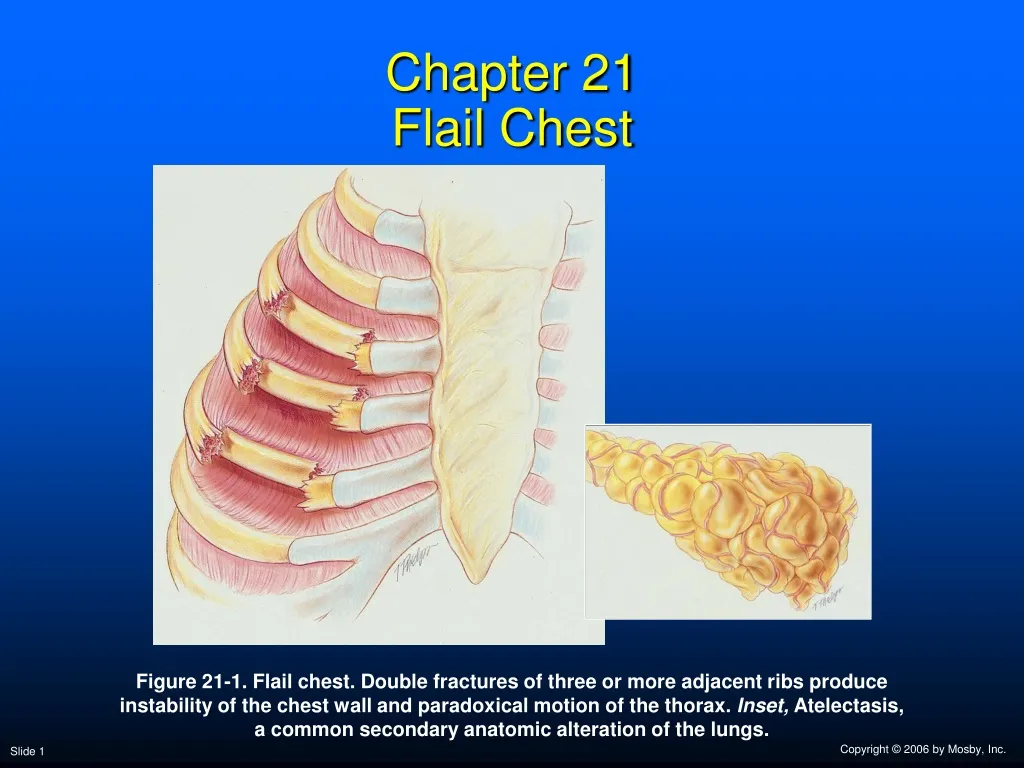
Chapter 21 Flail Chest. Figure 21-1. Flail chest. Double fractures of three or more adjacent ribs produce instability of the chest wall and paradoxical motion of the thorax. Inset, Atelectasis, a common secondary anatomic alteration of the lungs. Anatomic Alterations of the Lungs.

E N D
Chapter 21Flail Chest Figure 21-1. Flail chest. Double fractures of three or more adjacent ribs produce instability of the chest wall and paradoxical motion of the thorax. Inset, Atelectasis, a common secondary anatomic alteration of the lungs.
Anatomic Alterations of the Lungs • Double fracture of numerous adjacent ribs • Rib instability • Lung restriction • Atelectasis • Lung collapse • Lung contusion • Secondary pneumonia
Etiology • Direct compression by a heavy object • Automobile accident • Industrial accident
Overview of the Cardiopulmonary Clinical Manifestations Associated with FLAIL CHEST The following clinical manifestations result from the pathophysiologic mechanisms caused (or activated) by Atelectasis (see Figure 9-7) and Pneumonic Consolidation (see Figure 9-8)—the major anatomic alterations of the lungs associated with flail chest (see Figure 21-1).
Clinical Data Obtained at the Patient’s Bedside Vital signs • Increased respiratory rate • Stimulation of peripheral chemoreceptors • Other possible mechanisms • Decreased lung compliance • Activation of the deflation receptors • Activation of the irritant receptors • Stimulation of the J receptors • Pain/anxiety • Increased heart rate, cardiac output, blood pressure
Figure 21-2. Lateral flail chest with accompanying pendelluft.
Clinical Data Obtained at the Patient’s Bedside • Paradoxic movement of the chest wall • Cyanosis • Chest assessment findings • Diminished breath sounds • On the affected as well as the unaffected side
Clinical Data Obtained from Laboratory Tests and Special Procedures
Pulmonary Function Study: Lung Volume and Capacity Findings VT RV FRC TLC N or VC IC ERV RV/TLC% N
Arterial Blood Gases Mild to Moderate Flail Chest • Acute alveolar hyperventilation with hypoxemia pH PaCO2 HCO3- PaO2 (Slightly)
Time and Progression of Disease Disease Onset Alveolar Hyperventilation 100 90 Point at which PaO2 declines enough to stimulate peripheral oxygen receptors 80 70 60 PaO2 PaO2 or PaCO2 50 40 30 PaCO2 20 10 0 Figure 4-2. PaO2 and PaCO2 trends during acute alveolar hyperventilation.
Arterial Blood Gases Severe Flail Chest • Acute ventilatory failure with hypoxemia pH PaCO2 HCO3- PaO2 (Slightly)
Time and Progression of Disease Disease Onset Alveolar Hyperventilation Acute Ventilatory Failure 100 Point at which disease becomes severe and patient begins to become fatigued 90 Point at which PaO2 declines enough to stimulate peripheral oxygen receptors 80 70 PaCO2 Pa02 or PaC02 60 50 40 30 PaO2 20 10 0 Figure 4-7. PaO2 and PaCO2 trends during acute ventilatory failure.
Oxygenation Indices QS/QT DO2 VO2 C(a-v)O2 Normal (severe) O2ER SvO2
Hemodynamic Indices (Severe Flail Chest) CVP RAP PAPCWP CO SV SVICI RVSWI LVSWI PVRSVR
Radiologic Findings Chest radiograph • Increased density • Rib fractures
Figure 21-4. A, Chest X-ray film of a 20-year-old female with a severe right-sided flail chest. B, Close-up of the same X-ray film, demonstrating rib fractures (arrows).
General Management of Flail Chest Mild cases • Medication for pain and routine bronchial hygiene Severe cases • Volume-controlled ventilation with PEEP • 5 to 10 days usually adequate for sufficient bone healing
General Management of Flail Chest Respiratory care treatment protocols • Oxygen therapy protocol • Hyperinflation therapy protocol • Mechanical ventilation protocol