Download
1 / 1
10 likes | 441 Views
SMOKING CESSATION TREATMENT AT COMMUNITY BASED SUBSTANCE ABUSE REHABILITATION PROGRAMS: IMPACT ON CIGARETTE SMOKING.

E N D
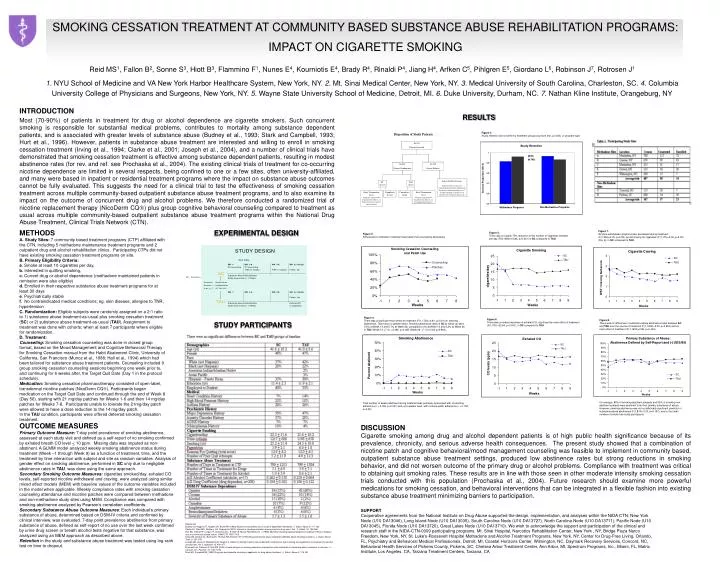
SMOKING CESSATION TREATMENT AT COMMUNITY BASED SUBSTANCE ABUSE REHABILITATION PROGRAMS: IMPACT ON CIGARETTE SMOKING Reid MS1, Fallon B2, Sonne S3, Hiott B3, Flammino F1, Nunes E4, Kourniotis E4, Brady R4, Rinaldi P4, Jiang H4, Arfken C5, Pihlgren E5, Giordano L6, Robinson J7, Rotrosen J11. NYU School of Medicine and VA New York Harbor Healthcare System, New York, NY. 2. Mt. Sinai Medical Center, New York, NY. 3. Medical University of South Carolina, Charleston, SC. 4. Columbia University College of Physicians and Surgeons, New York, NY. 5. Wayne State University School of Medicine, Detroit, MI. 6. Duke University, Durham, NC. 7. Nathan Kline Institute, Orangeburg, NY INTRODUCTION Most (70-90%) of patients in treatment for drug or alcohol dependence are cigarette smokers. Such concurrent smoking is responsible for substantial medical problems, contributes to mortality among substance dependent patients, and is associated with greater levels of substance abuse (Budney et al., 1993; Stark and Campbell, 1993; Hurt et al., 1996). However, patients in substance abuse treatment are interested and willing to enroll in smoking cessation treatment (Irving et al., 1994; Clarke et al., 2001; Joseph et al., 2004), and a number of clinical trials have demonstrated that smoking cessation treatment is effective among substance dependent patients, resulting in modest abstinence rates (for rev. and ref. see Prochaska et al., 2004). The existing clinical trials of treatment for co-occurring nicotine dependence are limited in several respects, being confined to one or a few sites, often university-affiliated, and many were based in inpatient or residential treatment programs where the impact on substance abuse outcomes cannot be fully evaluated. This suggests the need for a clinical trial to test the effectiveness of smoking cessation treatment across multiple community-based outpatient substance abuse treatment programs, and to also examine its impact on the outcome of concurrent drug and alcohol problems. We therefore conducted a randomized trial of nicotine replacement therapy (NicoDerm CQ) plus group cognitive behavioral counseling compared to treatment as usual across multiple community-based outpatient substance abuse treatment programs within the National Drug Abuse Treatment, Clinical Trials Network (CTN). RESULTS Figure 2. Study retention did not differ by treatment groups (log-rank test, p=0.28), or program type. . METHODS A. Study Sites: 7 community based treatment programs (CTP) affiliated with the CTN, including 5 methadone maintenance treatment programs and 2 outpatient drug and alcohol rehabilitation clinics. Participating CTPs did not have existing smoking cessation treatment programs on site. B. Primary Eligibility Criteria: a. Smoke at least 10 cigarettes per day, b. Interested in quitting smoking, c. Current drug or alcohol dependence (methadone maintained patients in remission were also eligible) d. Enrolled in their respective substance abuse treatment programs for at least 30 days e. Psychiatrically stable f. No contraindicated medical conditions; eg. skin disease, allergies to TNR, hypertension C. Randomization: Eligible subjects were randomly assigned on a 2:1 ratio to 1) substance abuse treatment-as-usual plus smoking cessation treatment (SC) or 2) substance abuse treatment-as-usual (TAU). Assignment to treatment was done with cohorts; when at least 7 participants where eligible for randomization. D. Treatment: Counseling: Smoking cessation counseling was done in closed group format, based on the Mood Management and Cognitive Behavioral Therapy for Smoking Cessation manual from the Habit Abatement Clinic, University of California, San Francisco (Munoz et al., 1988; Hall et al., 1994) which had been tailored for substance abuse treatment patients. Counseling included 9 group smoking cessation counseling sessions beginning one week prior to, and continuing for 6 weeks after, the Target Quit Date (Day 1 in the protocol schedule). Medication: Smoking cessation pharmacotherapy consisted of open-label, transdermal nicotine patches (NicoDerm CQ). Participants began medication on the Target Quit Date and continued through the end of Week 8 (Day 56), starting with 21 mg/day patches for Weeks 1-6 and then 14 mg/day patches for Weeks 7-8. Participants unable to tolerate the 21mg/day patch were allowed to have a dose reduction to the 14 mg/day patch. In the TAU condition, participants were offered deferred smoking cessation treatment. EXPERIMENTAL DESIGN Figure 7. Nicotine withdrawal symptoms also decreased during treatment (F(1,346)=4.03, p<0.05), as did craving for cigarettes (F(1,175)=5.02, p<0.05) (Fig. 6), in SC compared to TAU. Figure 5. There was a roughly 75% reduction in the number of cigarettes smoked per day (F(8,1084)=10.84, p<0.001) in SC compared to TAU. Figure 3. Adherence to medication treatment was better than counseling attendance. BD = Blood Draw, SM = Subjective Measure, EO = Eyes-Open EEG, EC = Eyes-Closed EEG Figure 4. There was a significant main effect of treatment (F(1,1724)=2.81, p<0.01) on smoking abstinence. There was no gender effect. Smoking abstinence rates in SC at follow-up were 5.5% at Week 13 and 5.7% at Week 26, compared to 0% at Week 13 and 5.2% at Week 26 in TAU (Week 13: c2 (1) =3.395, p=0.065; Week 26: c2 (1)=0.002 p=0.963). Figure 6. There was a modest decrease in exhaled CO, significant by main effect of treatment (F(1,751)=22.64, p<0.001), in SC compared to TAU. Figure 8. There was no difference in substance abuse abstinence rates between SC and TAU over the course of treatment (F(1,1632)=0.00, p=0.955) and no main effect of treatment (F(1,1633)=0.82, p=0.444). STUDY PARTICIPANTS On average, 85% of smoking abstinent subjects and 55% of smoking non-abstinent subjects were abstinent from their primary substance of abuse. However, smoking abstinence was not a statistically significant predictor of substance abuse abstinence (F(1,874)=2.00, p=0.157), due to the small number of smoke free study participants. Total number of weeks abstinent during treatment was positively associated with counseling adherence (r = 0.306, p<0.001) and, at a weaker level, with nicotine patch adherence (r = 0.152, p<0.05). OUTCOME MEASURES Primary Outcome Measure: 7-day point prevalence of smoking abstinence, assessed at each study visit and defined as a self-report of no smoking confirmed by exhaled breath CO level < 10 ppm. Missing data was imputed as non-abstinent. A GLMM model analyzed weekly smoking abstinence status during treatment (Week –1 through Week 9) as a function of treatment, time, and the treatment by time interaction with subject and site as random variables. Analysis of gender effect on smoking abstinence, performed in SC only due to negligible abstinence rates in TAU, was done using the same approach. Secondary Smoking Outcome Measures: cigarettes smoked/day, exhaled CO levels, self-reported nicotine withdrawal and craving, were analyzed using similar mixed effect models (MEM) with baseline values of the outcome variables included in the model when applicable. Weekly compliance rates with smoking cessation counseling attendance and nicotine patches were compared between methadone and non-methadone study sites using MEM. Compliance was compared with smoking abstinence analyzed by Pearson’s correlation coefficients. Secondary Substance Abuse Outcome Measures: Each individual’s primary substance of abuse, determined based on DSM-IV criteria and confirmed by clinical interview, was evaluated. 7-day point prevalence abstinence from primary substance of abuse, defined as self-report of no use over the last week confirmed by urine drug screen or breath alcohol tests negative for that substance, was analyzed using an MEM approach as described above. Retention in the study and substance abuse treatment was tested using log-rank test on time to dropout. DISCUSSION Cigarette smoking among drug and alcohol dependent patients is of high public health significance because of its prevalence, chronicity, and serious adverse health consequences. The present study showed that a combination of nicotine patch and cognitive behavioral/mood management counseling was feasible to implement in community based, outpatient substance abuse treatment settings, produced low abstinence rates but strong reductions in smoking behavior, and did not worsen outcome of the primary drug or alcohol problems. Compliance with treatment was critical to obtaining quit smoking rates. These results are in line with those seen in other moderate intensity smoking cessation trials conducted with this population (Prochaska et al., 2004). Future research should examine more powerful medications for smoking cessation, and behavioral interventions that can be integrated in a flexible fashion into existing substance abuse treatment minimizing barriers to participation. SUPPORT Cooperative agreements from the National Institute on Drug Abuse supported the design, implementation, and analyses within the NIDA CTN: New York Node (U10 DA13046), Long Island Node (U10 DA13035), South Carolina Node (U10 DA13727), North Carolina Node (U10 DA13711), Pacific Node (U10 DA13045), Florida Node (U10 DA13720), Great Lakes Node (U10 DA13710). We wish to acknowledge the support and participation of the clinical and research staff in the NIDA-CTN-0009 participating programs. Mt. Sinai Hospital, Narcotics Rehabilitation Center, New York , NY, Bridge Plaza Narco Freedom, New York, NY, St. Luke’s-Roosevelt Hospital Methadone and Alcohol Treatment Programs, New York, NY, Center for Drug-Free Living, Orlando, FL, Psychiatry and Behavioral Medical Professionals, Detroit, MI, Coastal Horizons Center, Wilmington, NC, Daymark Recovery Services, Concord, NC, Behavioral Health Services of Pickens County, Pickens, SC, Chelsea Arbor Treatment Center, Ann Arbor, MI, Spectrum Programs, Inc., Miami, FL, Matrix Institute, Los Angeles, CA, Tarzana Treatment Centers, Tarzana, CA References Budney AJ, Higgins ST, Hughes JR, Bickel WK (1993) Nicotine and caffeine use in cocaine-dependent individuals. J. Subst. Abuse 5, 117-130. Clarke JG, Stein MD, McGarry, KA, Gogineni A (2001) Interest in smoking cessation among injection drug users. Am. J. Addict. 10, 159-166. Hurt RD, Offord KP, Crogan IT, Gomez-Dahl L, Kottke TE, Morse RM, Melton III, J (1996) Mortality following inpatient addictions treatment: Role of tobacco use in a community-based cohort. JAMA 275, 1097-1103. Irving LM, Seidner AL, Burling TA, Thomas RG, Brenner GF (1994) Drug and alcohol abuse inpatient’s attitudes about smoking cessation. J. Subst. Abuse Treat. 6, 267-278. Joseph AM, Lexau B, Willenbring M, Nugent S, Nelson D (2004a) Factors associated with readiness to stop smoking among patients in treatment for alcohol use disorder. Am J. Addiction 13, 405-417. Prochaska JJ, Delucchi K, Hall SM (2004) A meta-analysis of smoking cessation interventions with individuals in substance abuse treatment or recovery. J. Consult. Clin. Psychol. 72, 1144-1156. Stark MJ, Campbell BK (1993) Drug use and cigarette smoking in applicants for drug abuse treatment. J. Subst. Abuse 5, 175-181.