Download
1 / 90
1.11k likes | 2.26k Views
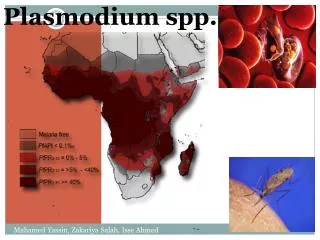
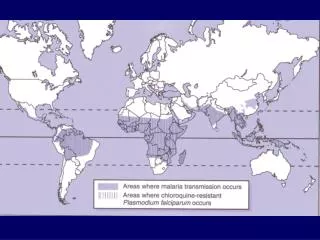
Malaria. Plasmodium falciparum Plasmodium vivax Plasmodium ovale Plasmodium malariae. 1. Malaria geographic distribution. 2. Malaria: Case-1.

E N D
Malaria • Plasmodium falciparum • Plasmodium vivax • Plasmodium ovale • Plasmodium malariae 1
Malaria: Case-1 On January 11, 2001, a 12 year-old resident of Michigan was taken to a clinic with a 2-day history of fever with chills, malaise, fatigue, cough and one episode of vomiting. At the clinic, the patient had a temperature of 102º F (39º C). The clinician noted that the patient had returned from Africa on January 6. Upper respiratory tract infection was diagnosed with nausea and vomiting, and the patient was prescribed an oral cephalosporin antibiotic and antiemetic agent. 3
Malaria: Case-1, continued The symptoms continued and on January 14, the patient collapsed, was transported to a local hospital, and died in the emergency department shortly thereafter. Examination of a peripheral blood film on stored blood from January 11 and a film from blood taken on January 14 demonstrated Plasmodium falciparum parasites with 0.8% parasitemia and 14 %, respectively. The patient’s mother also had P. falciparum malaria diagnosed in January, and later recovered. Both mother and son had taken chloroquine prophylactically. 4
Malaria: Case-2 On March 7, 2001, a 47-year-old resident of Minnesota returned to the US after 11 days in east Africa. Chloroquine was taken before and during the trip and proquanil was added on arrival in Africa. On returning to the US, proquanil was discontinued, and on March 11, the scheduled dose of chloroquin was taken. On March 17, the patient developed a persistent headache and on March 19, sought care for headache and dark urine at a Florida hospital emergency department. On admission, the patient’s temperature was 102º F (39º C); physical examination did not reveal any abnormalities. 5
Malaria: Case-2, continued A thick blood smear film obtained on admission was read as Plasmodium species, and later was confirmed as P. falciparum. The patient was admitted and treated with oral quinine and doxycycline; however, the patient developed cerebral edema and respiratory failure and died 6 days after admission. The patient had traveled to Africa with a group of 13 person; nine had taken mefloquine for prophylaxis and four had followed the same regimen as the patient. No other malaria cases were reported from the group. 6
Reported malaria cases in 2006 USA: 1,564 (six fatal) South Carolina: 8 South-East: 41 7
Reported indigenous malaria cases in the different states (1957-2003) 9
Species of indigenous malaria cases reported in the US (1957-2003) 10
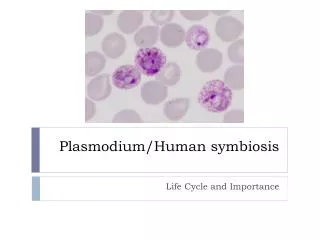
Malarial parasites morphology • Malignant tertian • Benign tertian • Ovale tertian • Quartan 11
type organ Involved symptoms Tertian (vivax and ovale) Headache, lassitude, vague aching of bones and joints, chills and high fever (103-106 F), nausea and vomiting, convulsion, euphoria, profuse sweating. Symptoms every other day and last 8-12 hours . Spontaneous recovery Spleen, liver, erythrocytes systemic falciparum (malignant tertian) Same as above but no tertian pattern: there may be daily spiking; no spontaneous recovery and ultimately fatal. Renal & CNS involvement quartan (malariae) Same as tertian, but paroxysm occurs every three days (2 clear days) Malarial symptoms 13
v f o m Malarial diagnosis • Travel history • symptoms • Blood smear 15
Malariacontrol and treatment • Control • Control mosquito population • Mosquito netting • Treatment: • Chloroquine • P. falciparum often drug resistant, but other drug choices are available 16
Chloroquine: mechanism of action Chloroquine is a 4-aminoquinoline Inside the red blood cells malaria parasite digests hemoglobin and produces heme which is toxic to the parasite To prevent the toxicity, parasite biocrystallizes heme to form hemozoin which is non-toxic Chloroquine enters the red blood cells, prevents the process of biocrystallization, that leads to accumulation of heme and death of parasite 17
Babesiosisgeography andetiology • Etiologic agent is Babesia microti • Zoonotic infection • Deer are primary reservoir • Cases reported in north-eastern part of the US and Europe 18
Babesiosismorphology • Similar to malarial parasite, but no schizonts or gametocytes • Up to four trophozoites per cell, no sexual cycle 19
Babesiosissymptoms • Mild chills and fever • Hemolytic anemia • Jaundice • Hepatomegaly No malarial paroxysm 21
Babesiosisdiagnosis • Symptoms • History of tick bite No malarial paroxysm • Characteristic organisms in blood 22
Babesiosisprevention and treatment • Avoid tick bites • Recovery may be spontaneous • Clindamycin with quinine is effective 23
Toxoplasmosis • The etiologic agent T.gondii is distributed worldwide • Most of the populations is seropositive • Threat to immunosuppressed and unborn 24
Toxoplasmagondiimorphology • Intracellular (macrophage) parasite • 3-6 x 1-2 µm 25
host status symptoms Prenatal 1-5% aborted, 8-10% serious brain and eye damage, 10-13% less serious visual and mental problems, ~70% late visual and mental problems Normal adult Flu-like Immuno-compromised Parasitemia, cysts in visceral organs, eye, and CNS, often fatal Toxoplasmosissymptoms 27
Toxoplasma gondiiPathology and Immunology Pathology • Growingmass • CMI Immunology • Both humoral and CMI are stimulated • CMI is protective 31
Toxoplasma gondiiDiagnosis and treatment Diagnosis • History • CT scan • Tonsil or lymph node biopsy Treatment • Sulphonamide or pyrimethamine Spiramycin 32
Pneumocystiscarinii Not a protozoan, it’s a yeast • Opportunistic • Major cause of pneumonia among AIDS patients Treatment • trimethoprim • sulphamethoxazole 33
Facultative protozoan parasites Negleria Fowleri • Rare • In warm spas • Causes encephalitis Acanthamoeba • Rare • In soil • pharyngitis, occasionally encephalitis 34
Amebiasis • Etiologic agent: • Entamoeba histolytica • Disease: • Amoebic dysentery • Liver, lung, brain and other abscesses 1
Fecal-oral life cycle Excystation Trophozoite Cyst Encystment Passed in feces Metabolically active 2
Organ involved Symptoms Symptoms of acute amebiasis Abdominal pain; frequent bloody dysentery with necrotic mucosa Small and large intestine 3
Organ involved Symptoms Symptoms of chronic amebiasis Small and large intestine Recurrent bloody and mucoid dysentery Abscess; hepatitis Liver Abscess; pneumonia Lung Abscess; encephalitis Brain 4
E. Histolytica:pathology Pathology Invasiveness and abscess formation are due to amoebic proteolytic enzymes 5
Amebiasis:Differential diagnosis Amebiasis is different from giardiasis and bacterial dysentery Mucus and blood in stool No granulocytosis No high fever 6
E. Histolytica:the diagnostic features When amebic dysentery is suspected, a fresh fecal sample or a swab should be examined under microscope. If examined quickly the colorless motile trophozoite can be seen. H/E stained Fresh sample 7
E. Histolytica:treatment • Treatment • Iodoquinol for acute amebiasis • Metronidazole for chronic amebiasis 8
Giardiasis • Etiologic agent: Giardialamblia • Diarrhea, lipid and vitamin B12 and other nutrient mal-absorption 9
organ involved symptoms stage Acute Small and large intestine Flatulence; foul-smelling, bulky light diarrhea; malabsorption, lactose intolerance Chronic Small and large Intestine Asymptomatic or symptoms described above Giardiasis: symptoms 10
Giardiasis: pathology Pathology • Covering of the epithelium by trophozoites and flattening of the mucosal surface (no invasiveness) 11
Giardiasis: Differential diagnosis Giardiasis is different from amebiasis and bacterial dysentery: No mucus, blood No granulocytosis and no fever 12
Giardiasis: diagnosis The mainstay of diagnosis of Giardia is stool microscopy, this can be for distinctive oval cyst and motile trophozoite 13
Giardiasis: treatment • Treatment • Iodoquinol • Metronidazole 14
Balantidium coli • Primarily a zoonotic intestinal parasite: • Horses, cows, pigs • Farm workers at risk • Symptoms similar to amebiasis except, No abscesses in peripheral organs 15