Download
1 / 70
790 likes | 1.72k Views
Anatomy and Injuries of the Knee. Connie Rauser Sabino Sports Medicine. Anatomy-Bones. Bones Femur Medial/lateral femoral condyles articulate w/ tibia Tibia Tibial plateau is flat-articulates w/ femoral condyles Fibula Articulates w/ tibia Patella Sesamoid bone protects anterior joint

E N D
Anatomy and Injuries of the Knee Connie Rauser Sabino Sports Medicine
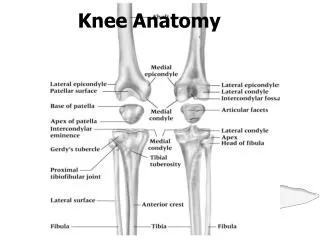
Anatomy-Bones • Bones • Femur • Medial/lateral femoral condyles articulate w/ tibia • Tibia • Tibial plateau is flat-articulates w/ femoral condyles • Fibula • Articulates w/ tibia • Patella • Sesamoid bone protects anterior joint • Enclosed in quadriceps/patellar tendon
Anatomy-Joints • Joints • Tibiofemoral • Hinge joint with synovial lining • diarthrodial • Patellofemoral • Superior Tibiofibular
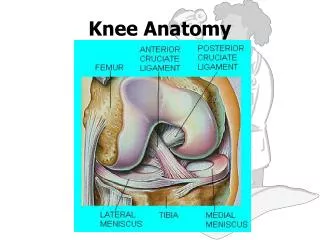
Anatomy-Meniscus • Meniscus • Medial and lateral • Fibrocartilaginous disks • Thicker on outside than inside (poor blood supply) • Lie on top of tibial plateau • Increase stability • Make condyles fit better • Shock absorbers
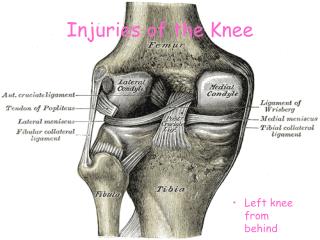
Anatomy-Ligaments • ACL-anterior cruciate ligament • Runs from anterior tibia to posterior femur • Prevents anterior displacement of tibia on fixed femur • Prevents femur from moving posterior during weight bearing • Stabilizes tibia against excessive internal rotation
Ligaments • PCL-posterior cruciate ligament • Runs from posterior tibia to anterior femur • Prevents posterior translation of tibia on fixed femur • Prevents femur from moving anterior during weight bearing • Both ACL and PCL “cross” or wrap around each other—taut when in extension and looser when in flexion
Ligaments • MCL-medial collateral ligament • Attaches on the medial femoral epicondyle & anteromedial tibia • Thickened portion of joint capsule • Two parts-superficial and deep • Deep portion attaches to medial meniscus • Stabilizes against valgus stress applied to lateral aspect of joint capsule
Ligaments • LCL-lateral collateral ligament • Attaches to lateral femoral epicondyle and head of fibula • Stabilizes against varus stress when force is applied to medial aspect of joint • Both the MCL and LCL are tightest during full extension of knee and relaxed during flexion
Muscles • Quadriceps • Rectus femoris, vastus lateralis, vastus medialis, vastus intermedius • Knee extension, hip flexion • Hamstrings • Biceps femoris, semimembranosus, semitendinosus • Knee flexion, hip extension
Muscles • Gracilis • Knee flexion, hip adduction • Sartorius • Knee flexion, hip flexion, hip external rotation • Popliteus • Knee flexion • Gastrocnemius • Knee flexion
Muscles • Plantaris • Knee flexion • Pes anserine • Goose’s foot • Knee flexion, some internal rotation • Gracilis, sartorius, semitendinosus • Iliotibial Band • Thick band on lateral aspect of thigh • Attaches at Gerdy’s tubercle on the lateral aspect of tibia
Preventing knee injuries • Conditioning • Strength, flexibility, cardiovascular and muscular endurance • Hamstring strength 60% of quad strength • Rehabilitation • Strengthen all muscles around knee joint • Shoes • proper type for surface • Length of cleats • Turf vs grass
Preventing knee injuries • Knee braces • Functional vs. prophylactic • Functional—used to provide support to an unstable knee • Usually custom fitted to some degree • Uses hinges and supports to control excessive rotational stress and tibial translation • Prophylactic-worn on lateral aspect knee to protect MCL. • Usefulness questioned—does it cause more injuries?
ACL rupture • Mxn: • fixed foot and external rotation of femur • knee in valgus position • hyperextension • S/S: • “pop”, • knee gives out • instability of knee joint • swelling within knee joint—hemarthrosis • intense pain initially but still able to walk • “+” Lachman’s test • “+” anterior drawer test
MXN • Hyperextension
Inside the knee joint • The ACL intact The ACL torn
ACL Rupture • Tx: RICE, knee immobilizer, crutches, Physician referral • Requires surgical reconstruction • Timing of surgery decided by athlete, parents, doctor • Grafts used are patellar tendon, hamstring tendon, cadaver graft, allograft • 3-5 weeks in brace, 6-9 months return to activity
Stress tests • Lachman’s test
Stress tests • Modified Lachman’s
Stress tests • Anterior Drawer test
PCL Rupture • Mxn: • hyperflexion • falling on bent knee with foot plantar flexed • Hit on fixed anterior tibia • S/S: • “pop” at the back of knee • POT and swelling in popliteal fossa • + posterior sag test, +sunrise test, + posterior drawer test
PCL rupture • Tx: • RICE • Immobilization • Crutches • Physician referral • 6-8 weeks rest/rehab • If surgery is elected, 6 weeks immobilization
Stress tests • Posterior sag
Strest tests • Sunrise or posterior sag
MCL Sprain • Mxn: • Blow to the lateral side of knee (valgus stress) • External rotation of tibia
MCL sprain • 2nd degree??
MCL sprain • S/S: • 1st degree • POT over MCL, stable but pain with valgus stress, mild joint effusion, mild joint stiffness, full ROM • 2nd degree • Partial tearing-superficial portion, POT over MCL, some instability with valgus stress but solid endpoint, moderate joint effusion, joint stiffness, limited ROM, unable to fully extend knee joint
MCL Sprain • S/S: • 3rd degree • Complete tear—superficial and deep portions • POT over MCL • Moderate to severe effusion • Severe pain • Loss of motion due to pain, effusion, muscle guarding • “+” valgus stress in 0 and 30 degrees, no endpoint
Stress tests for MCL • Valgus stress test @ 0 Valgus stress @ 30
MCL Sprain • Tx: • RICE • Crutches • Knee immobilizer/brace • 1st degree 1-2 weeks • 2nd degree 2-4 weeks • 3rd degree 4-6 weeks • Physician referral for 2nd degree or greater
Complications • The terrible triad or unhappy triad • Torn ACL • Torn MCL • Torn Medial meniscus
LCL sprain • Mxn: • Varus force to medial aspect of knee • internal rotation of tibia • S/S: • POT over LCL, • pain, • swelling, • loss of motion, • “+” varus stress at 30 degrees—solid endpoint with 1st degree, less stability but solid endpoint with 2nd degree, no endpoint with 3rd degree • if “+” varus stress at 0 degrees flexion suspect ACL or PCL injury as well
LCL sprain • Tx: • RICE • Crutches • Knee immobilizer • Physician referral with 2nd or 3rd degree
Meniscus tear • Medial: more often torn than later due to attachment to MCL • Lateral: doesn’t attach to joint capsule making it more mobile, less prone to injury • Mxn: • Weight bearing with rotational force while extending or flexing the knee
Meniscus tear • S/S: • Effusion w/in 48-72 hours • POT over joint line • Loss of motion • “locking” • Giving out • Pain with deep knee flexion--squatting
Meniscus tear • Types of meniscus tears
Meniscus tears • Tx: • RICE • Crutches if necessary • Physician referral • If knee is “locked” by displaced meniscus, go to ER • Arthroscopic surgery to fix
Injuries to the Patella • Dislocation • Subluxation • Fracture • Chondromalacia • Patellar tendonitis
Patella Dislocation • Mxn: • Foot planted, deceleration, and cutting in opposite direction from the weight bearing foot • Thigh rotates internally while leg rotates externally • Strong forceful contraction of quads (vastus lateralis)
Dislocation • S/S: loss of motion/function at the knee • Pain • Swelling • Deformity • POT over medial aspect of knee joint
Dislocation • Tx: • immobilize in position you find it • Ice • ER visit • After reduction, immobilize in extension about 4 weeks—use crutches • Strengthen muscles of knee, thigh and hip
Patella Subluxation • Mxn: same as for the dislocation • S/S: • same as for the dislocation except there will be no deformity • POT over the medial knee joint • Pain with movement • TX: • RICE • Knee Immobilizer and crutches • Physician referral
Patella fracture • Mxn: • direct impact or trauma to patella • Indirect trauma in which a severe pull of the patellar tendon occurs against the femur when the knee if semi-flexed • S/S: • hemorrhage which results in significant swelling • pain • POT over Patella • extreme pain with weight bearing/movement