Download
1 / 18
180 likes | 447 Views
Asthma Stability Model for Inhaled Corticosteroid Dose-Response. Wallace P. Adams, PhD OGD/OPS/CDER/US FDA Advisory Committee for Pharmaceutical Science and Clinical Pharmacology 23 July 2008. Outline of the Presentation. Methods to establish BE Challenges to ICS BE

E N D
Asthma Stability Model for Inhaled CorticosteroidDose-Response Wallace P. Adams, PhD OGD/OPS/CDER/US FDA Advisory Committee for Pharmaceutical Science and Clinical Pharmacology 23 July 2008
Outline of the Presentation • Methods to establish BE • Challenges to ICS BE • Asthma stability model: Pilot study • crossover vs parallel design • estimates of sample size for a BE study • Asthma stability model: FDA research • Pharmacodyamic study data analysis
Methods for Establishment of BE • In vivo studies in humans comparing drug or active metabolite in an accessible biologic fluid • In vivo studies in humans comparing a pharmacodynamic endpoint • Comparative clinical trials to demonstrate BE • Comparative in vitro studies 21 CFR 320.24(b)
Response Equivalence DOSE-RESPONSE Reduced safety Reducedefficacy Adapted from JN Pritchard, ANZSRS Annual Meeting, Brisbane, 16-19 Mar 2001
Inhaled Corticosteroids (ICS) • Dose-response* • Differences from placebo for each active dose are statistically significant • A dose-response generally exists • shallow • Lack of statistical significance in response between adjacent doses • high variability of response • 4-fold or greater dose differences generally required to detect statistical significance • Carryover between treatment periods is a concern for crossover study designs • Unequal carryover can bias the estimate of difference between treatment means *PJ Barnes et al, AJRCCM 1998;157:S1-53
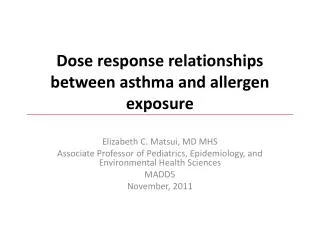
Dose-Response (D-R): CFC vs HFA Beclomethasone Dipropionate • Subjects • age >18 yrs with asthma • 50-75% of predicted • N=50-59 per treatment • Treatments • BDP for 6 weeks • Parallel group design • Up to 28 day ICS washout • with placebo MDI • 100, 400 or 800 mcg daily • (BID dosing), blinded to • dose WW Busse et al, JACI 1999;104:1215-22
Dose-Response (D-R): CFC-BDP and HFA-BDP WW Busse et al, JACI 1999;104:1215-22
Relative Potency of CFC-BDP and HFA-BDP (Finney Bioassay Method) WW Busse et al, JACI 1999;104:1215-22, cited in JA Vanden Burgt et al, JACI 2000;106:1209-1226
Asthma Stability after Oral Prednisone Model • Pilot study in 12 adult asthmatics • Randomized two period crossover study • Oral prednisone (40 mg BID) wash-in, 4-7 days • Two doses of HFA-BDP; 100, 800 mcg/day • 21 day treatment period with ICS • Periodic measurement of pulmonary function • Repeat wash-in (4-7 day), crossover ICS (21 day) RC Ahrens et al, AJRCCM, 2001;164:1138-45
Sample Size Estimates(based on the Ahrens Pilot Study) • Assume • 2 by 2 study design (2 doses of each preparation) • Finney bioassay • 90% confidence interval • BE interval on the dose scale is 50 - 200% • power = 80% • parallel or crossover study design • Sample size estimates • based on ‘s’ and ‘b’ at end of treatment period • ‘s’ is SD for responses from ANOVA • ‘b’ is dose-response slope • low s/b ratio increases study power RC Ahrens et al, AJRCCM, 2001;164:1138-45
Mean Responses by Study Treatment Day Mean AM FEV1 Response s/b ratios RC Ahrens et al, AJRCCM, 2001;164:1138-45
Study Design: Parallel vs Crossover RC Ahrens et al, AJRCCM, 2001;164:1138-45
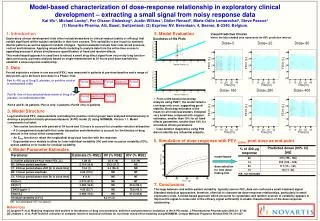
Asthma Stability Model:FDA Study Objectives • Oral prednisone versus high dose ICS • Effect on maximum FEV1 value during high dose run-in of each crossover treatment • Effect on observed D-R • Characterize D-R based on three treatment levels • Study efficiency of screening process for identifying subjects demonstrating sufficient D-R (study enrichment) • Examine D-R of primary and secondary outcome variables • Characterize D-R using linear, nonlinear and Emax modeling
Design and Conduct of the FDA Study • Subjects • Persistent asthma, non-smoking • Exhibit dose-response during run-in • Run-In Study Periods • 14 day high-dose ICS run-in (220 mcg x 4 actuations BID) • 28 day low-dose ICS run-in (44 mcg x 1 actuation BID) • Study Treatment Periods • high dose corticosteroid burst • oral prednisone on two periods, or • ICS • randomly assigned • 4 randomized crossover periods • double-blind, double-dummy • 28 days per period • 44 mcg (1 actuation) , 88 mcg (2 actuations), 88 mcg, and 352 (8 actuations) mcg BID
Design and Conduct of the Study 7 day prednisone or 14 day FP 7 day 14 day 28 day 28 day High dose run-in Low dose run-in Pre-study HDCB FP treatment 44, 88, 88, 352 mcg BID N = up to 120 (est.) N = 30 N = 24 • Home spirometry: AM FEV1 and PM FEV1 every day • Office spirometry at each clinical visit • eNO at each clinic visit
BE Criteria on the Dose Scale: Theory W Gillespie, ACPS Meeting, 16 Aug 1996
Dose Scale Approach to Estimate Relative BA Drug X (hypothetical example) for RLD 2 (180 mcg) puffs of RLD Dose of RLD that would result in a RLD RLD MDI Dose (mcg) Revised from W Gillespie, ACPS Meeting, 16 Aug 1996
Acknowledgments • Project Advisory Group • Badrul Chowdhury, MD, PhD, Division of Pulmonary and Allergy Products, OND • Sally Seymour, MD, DPAD • Robert Lionberger, PhD, OGD/OPS • Bing Li, PhD, OGD/OPS • Wallace Adams, PhD, OGD/OPS • Lawrence Yu, PhD, OGD/OPS