Download
1 / 58
600 likes | 1.25k Views
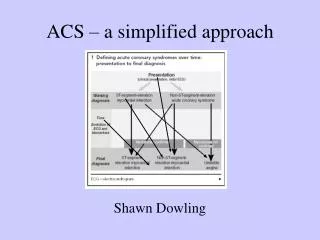
A Simplified Approach To ECHO Evaluation of CHF with Normal or Reduced EF. Anthony C. Pearson, MD, FACC 10/18/2008. Echo in CHF. Identifies Hypertrophic Cardiomyopathy and accurately measures LV Hypertrophy Excludes other causes of CHF or SOA Valvular disease (MR/MS, AS/AI)

E N D
A Simplified Approach To ECHO Evaluation of CHF with Normal or Reduced EF • Anthony C. Pearson, MD, FACC • 10/18/2008
Echo in CHF • Identifies Hypertrophic Cardiomyopathy and accurately measures LV Hypertrophy • Excludes other causes of CHF or SOA • Valvular disease (MR/MS, AS/AI) • Pericardial Effusion
Echo in CHF • Provides accurate Ejection Fraction • Every echo with interpretable images of LV function should have EF measured and reported out precisely along with end-diastolic and end-systolic volumes • Preferably biplane technique • When performed properly , echo EF is more reliable than cath EF or SPECT nuclear EF* Pearson, 2008, personal communication
Echo in CHF-Low EF • CHF with Reduced EF (EF < 50%) • Treatment with ACE inhibitors, Beta-blockers shown to reduce mortality, CHF hospitalizations and improve EF • CHF with Severely Reduced EF • Benefit from Device Therapy (ICD or Biventricular pacemaker)
ACC/AHA Guidelines-Device Based Therapy • We also acknowledge that the determination of LVEF lacks a "goldstandard" and that there may be variation among the commonlyused clinical techniques of LVEF determination. All clinicalmethods of LVEF determination lack precision, and the accuracyof techniques varies among laboratories and institutions. Onthe basis of these considerations, the present writing committeerecommends that clinicians use the LVEF determination that theybelieve is the most clinically accurate and appropriate in theirinstitution. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) Developed in Collaboration With the American Association for Thoracic Surgery and Society of Thoracic Surgeons
Class I Indications for ICD Therapy • 4 ICD therapy is indicated in patients with LVEF lessthan 35%due to prior myocardial infarction who are at least40 dayspost--myocardial infarction and are in NYHA functionalClassII or III. (Level of Evidence: A) (4,139) • 5 ICD therapyis indicated in patients with nonischemic dilatedcardiomyopathywho have an LVEF less than or equal to 35% andwho are in NYHAfunctional Class II or III. (Level of Evidence:B) (4,139–141) • 6 ICD therapy is indicated in patients with LV dysfunctiondueto prior myocardial infarction who are at least 40 dayspost--myocardialinfarction, have an LVEF less than 30%, andare in NYHA functionalClass I. (Level of Evidence: A) (4,132) • 7 ICD therapy is indicated in patients with nonsustained VTdue to prior myocardial infarction, LVEF less than 40%, andinducible ventricular fibrillation or sustained VT at electrophysiologicalstudy. (Level of Evidence: B) (4,131,142) ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) Developed in Collaboration With the American Association for Thoracic Surgery and Society of Thoracic Surgeons
Class IIB Indications for ICD Therapy Performed • 1 ICD therapy may be considered in patients with nonischemicheart disease who have an LVEF of less than or equal to 35%and who are in NYHA functional Class I. (Level of Evidence:C) • 2 ICD therapy may be considered for patients with long-QTsyndromeand risk factors for SCD. (Level of Evidence: B) (4,143–148) • 3 ICD therapy may be considered in patients with syncope andadvanced structural heart disease in whom thorough invasiveand noninvasive investigations have failed to define a cause.(Level of Evidence: C) • 4 ICD therapy may be considered inpatients with a familialcardiomyopathy associated with suddendeath. (Level of Evidence:C) • 5 ICD therapy may be consideredin patients with LV noncompaction.(Level of Evidence: C) ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) Developed in Collaboration With the American Association for Thoracic Surgery and Society of Thoracic Surgeons
Recommendations for Cardiac Resynchronization Therapy in PatientsWith Severe Systolic Heart Failure Class I 1 For patients who have LVEF less than or equal to 35%, a QRSduration greater than or equal to 0.12 seconds, and sinus rhythm,CRT with or without an ICD is indicated for the treatment ofNYHA functional Class III or ambulatory Class IV heart failuresymptoms with optimal recommended medical therapy. (Level ofEvidence: A) (222,224,225,231) Class IIa 1 For patients who have LVEF less than or equal to 35%, a QRSduration greater than or equal to 0.12 seconds, and AF, CRTwith or without an ICD is reasonable for the treatment of NYHAfunctional Class III or ambulatory Class IV heart failure symptomson optimal recommended medical therapy. (Level of Evidence:B) (220,231) 2 For patients with LVEF less than or equal to35% with NYHAfunctional Class III or ambulatory Class IV symptomswho arereceiving optimal recommended medical therapy and whohave frequentdependence on ventricular pacing, CRT is reasonable.(Levelof Evidence: C) (231) Class IIb 1 For patients with LVEF less than or equal to 35% with NYHAfunctional Class I or II symptoms who are receiving optimalrecommended medical therapy and who are undergoing implantationof a permanent pacemaker and/or ICD with anticipated frequentventricular pacing, CRT may be considered. (Level of Evidence:C) (231)
CHFREF • 84 year old male with remote history of MI and CABG • Progressively worsening SOA over last year with PND, orthopnea • BNP 988 • CXR-?LLL infiltrate, Cardiomegaly
Pearson’s Principle • Measure Reproducible Parameters which are simple and have direct clinical importance and do them on every patient. .
Two Key Diastolic Parameters to Measure • Peak Velocity of Early Mitral Inflow by Pulsed Doppler- (E) • Peak Early Velocity of Mitral Anulus by Tissue Doppler (E’)
Things I won’t Measure-either too laborious (TL) or not reproducible (NR) or Both (B) • Response of mitral flow to Valsalva (TL) • Pulmonary venous flow (TL) • M-mode Color Doppler of mitral inflow (NR) • Pulmonary Venous A wave (B) J Am Coll Cardiol 18:1, 65-71 (1991) Evaluation of pulmonary venous flow by transesophageal echocardiography in subjects with a normal heart: comparison with transthoracic echocardiography. Castello, R, Pearson, AC, Lenzen, P and Labovitz, AJ
Pulsed Tissue Doppler • Samples lower velocity myocardial motion at a particular site • Patterns similar to pulsed Doppler with a peak in early diastole (E’) and one corresponding to atrial systole (A’) • Most studied and useful measurements come from mitral anulus either medial or lateral
Alternative terms for peak early diastolic tissue velocity-Em, Ea, E’ • Alternative sites-medial,lateral,anterior,inferior anulus also measured and mid and apical sites in LV • Some studies average 2 or 4 sites, some use medial, some lateral, • Some studies use color tissue Doppler
Age-related Changes in “diastolic function” parameters derived from Echo/Dooppler
Scatter plot of peak early diastolic mitral annular velocity (E') versus {tau} Ommen, S. R. et al. Circulation 2000;102:1788-1794 Copyright ©2000 American Heart Association
E/E’ provides a reasonably accurate noninvasive way of measuring PCWP=LA Pressure Text Text Nagueh, et al 1997 A significant relation was observed between the early diastolic velocity (Ea) measured at the lateral border of the mitral annulus and the same velocity derived from the septal corner of the annulus (r = 0.88, p < 0.0001; lateral Ea = [1.05 × septal Ea] + 1.3). The lateral velocities were slightly higher than the septal velocities, as shown by the regression equation, and were often easier to quantify. For this reason, they were chosen for the rest of the statistical analysis.
asare tr RVSP=37 mm Hg +10 mm Hg=47 mm Hg
5 Things We Should Know After Each Echo • EF • LA Pressure (E/E’) • RA Pressure (IVC) • PA Pressure (TR, PV ) • LA volume
Results of Noninvasive Right Heart Cath • EF calculated as 16% with severe LVE • E/E’ of 34 (1.25)=LA pressure 42 mm Hg • RVSP calculated as 52 mm Hg (TR peak squared x 4 )plus 10-15 mm Hg for CVP (IVC plethora)=62-67 mm Hg • RAP estimated at 15 mm Hg (no collapse with sniff) • LAESVI=71 ml/m2=massively enlarged
CHF with Normal EF(HFNEF) • CHF best considered a single syndrome with a progressive decline in systolic performance
HF with normal EF or diastolic HF • Diastolic dysfunction present in CHF patients with low EF • CHF patients with normal EF have evidence of impaired systolic function • Unimodal distribution of EF
HF-Systolic or Diastolic? • CHF is a continuum -patients usually have varying degrees of both systolic and diastolic dysfunction contributing to symptoms • EF is a useful discriminator of types, just as ST elevation is for MI but it is not perfect and the EF cutoff is arbitrary • Thus, just as we have moved from terms transmural and nontransmural MI to ST elevation and non ST elevation MI we should be moving to HFNEF and HFREF
How to diagnose HFNEF Patient presents with signs or symptoms of CHF EF>50%, EDVI<97ml/m2 BNP, E/E’ E/E’ 8-15 BNP<200, E/E’<8 BNP<100 BNP 100-300 BNP>500 BNP>200, E/E’ >15 Not CHF DefiniteHFNEF Grey Zone (Higher #s increase probability of HFNEF)
CHF with Normal EF • About 50% of patients with CHF have normal EF • Patients are older, more likely female and hypertensive • Morbidity and Mortality appear similar to CHF patients with reduced EF (HFREF)
Does My Patient Have HFNEF? • 82 yo WF presents with recurrent breathlessness • Hx of hypertension, recent cath showing minimal CAD, normal EF • PE-no rales/no S3/no edema/no JVP • CXR-”NAD”
Does My Patient Have HFNEF? • Two Key Diagnostic Tests needed to answer the question • BNP • Properly performed and interpreted Echo/Doppler/tissue Doppler
Does My Patient Have CHF? BNP=475
Echo in CHF • Provides noninvasive “right heart cath” • Right ventricular systolic pressure or PA systolic pressure • RA pressure • Left atrial (LA) pressure, PCWP, LVEDP
Pulsed Doppler Peak Early Filling Velocity (E) = 1.23 M/s or 123 cm/s Pulsed Doppler E/A
Does My patient Have HFNEF? • HFNEF is characterized by elevated LV filling pressures which can be accurately estimated by Doppler/tissue Doppler techniques • Key parameter to measure is E/E’-the higher this value, the higher the patients LA pressure • The higher the patients LA pressure, the more HF signs and symptoms they will have
Diastolic filling of the left ventricle in a patient with hypertrophic cardiomyopathy. The high fidelity left ventricular (LV) and left atrial (LA) pressures are shown with a schematic representation of ascending aortic pressure (Ao). In the classic system, the cardiac cycle is divided into systole and four phases of diastole: isovolumetric relaxation (IVR), rapid filling (RF), slow filling (SF) and atrial contraction (AC). In a more practical and simplified system, the cardiac cycle is divided into contraction, relaxation and diastolic filling. Each of the three phases is dependent on effects of the preceding phase
Early Concepts of Diastolic function (circa 1985) • High E/A ratio good • Low E/A ratio bad • Low E/A=”stiff ventricle” or “reduced compliance”