Download
1 / 35
430 likes | 936 Views
HUMAN RABIES PREVENTION: PROPHYLAXIS MANAGEMENT. Charles E. Rupprecht VMD, MS, PhD Chief, Rabies Program PRB/DVRD/NCZVED/CCID/CDC. DEFINITION. Rabies is an acute, progressive encephalomyelitis The case to fatality rate is the highest of any infectious disease

E N D
HUMAN RABIES PREVENTION:PROPHYLAXIS MANAGEMENT Charles E. Rupprecht VMD, MS, PhD Chief, Rabies Program PRB/DVRD/NCZVED/CCID/CDC
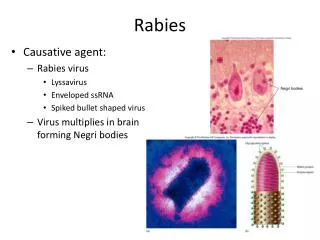
DEFINITION • Rabies is an acute, progressive encephalomyelitis • The case to fatality rate is the highest of any infectious disease • One of the oldest described diseases • The leading viral zoonosis as regards global public health significance
ETIOLOGY • Rabies is caused by RNA viruses in the family Rhabdoviridae, genus Lyssavirus • The type species of the genus is Rabies Virus • At least other 6 other lyssavirus species or genotypes cause rabies • Recently, 4 new lyssaviruses from Eurasian bats have been described as putative species
DISTRIBUTION • Rabies is distributed on all continents (with the exception of Antarctica) • Several areas are considered ‘free’ of the disease, including many islands in Pacific Oceania • Globalization may threaten the disease-free status of many localities, due to the introduction of rabid animals
RABIES HOSTS • All warm-blooded vertebrates are susceptible to experimental infection • Mammals are the natural hosts of rabies • Reservoirs consist of the Carnivora (canids, skunks, raccoons, mongoose, etc.) and Chiroptera (bats)
BURDEN • More than ~55,000 human rabies deaths per year • Most occur in developing countries • Millions of human exposures per year • The domestic dog is the single most important animal reservoir • Wildlife important, especially in developed countries
RABIES PATHOGENESIS • Virus is transmitted via bite • Agents are highly neurotropic • Enter peripheral nerves • Centripetal travel by retrograde flow in axoplasm of nerves to CNS • Replicate in brain • Centrifugal flow to innervated organs, including the portal of exit, the salivary glands • Viral excretion in saliva
RABIES DIAGNOSIS • Based upon history of animal exposure and typical neurological clinical signs • Postmortem demonstration of viral antigen in CNS is gold standard • In humans, antemortem detection of virus or viral amplicons, antibodies, or antigens (sera, csf, saliva, nuchal biopsy)
CLINICAL STAGES • Incubation Period (range = ~<7 days to >6 years; average is ~4-6 weeks) • Prodromal Phase (Non-specific signs) • Acute Neurological Phase • Coma • Death (recovery from rabies?)
RABIES RECOVERY? • Five historical human case recoveries, after vaccination, but before illness onset • Only one documented unvaccinated human survivor after clinical presentation
RABIES IN THE USA • Human rabies uncommon (1-8 cases per year); ~ 20,000 – 40,000 human exposures per year • Approximately 7,000 – 10,000 animal rabies cases diagnosed per year • Dog rabies transmission eliminated • Wildlife hosts include raccoons, skunks, foxes, mongoose (Puerto Rico), and bats • Distributed in every state except Hawaii
RABIES EXPOSURE • Bite (common cause) • Non-bite (rarely causes rabies) • Contacts with blood, urine, feces, etc. are not considered exposure • Many scenarios, such as merely seeing a rabid animal, being in the same room, petting, etc., are not considered grounds for prophylaxis A small bat bite on a finger
PROPHYLAXIS • Pre-exposure Vaccination • Postexposure Prophylaxis (PEP)
PRE-EXPOSURE VACCINATION • Provided to subjects at risk before occupational or vocational exposure to rabies • Subjects include diagnosticians, laboratory & vaccine workers, veterinarians, cavers, etc. • Simplifies postexposure management
POSTEXPOSURE PROPHYLAXIS • Provided to subjects after rabies exposure • Consists of wound care, rabies immune globulin, and vaccine • If prompt and proper, survival virtually assured
RABIES BIOLOGICALS • Rabies Vaccines (for pre- and PEP) • Rabies immune globulin (only in PEP)
RABIES VACCINES • Two Human Rabies Vaccines in USA: Human Diploid Cell Vaccine Imovax® (HDCV) Purified Chick Embryo Cell RabAvert® (PCEC) • RVA no longer available • Intradermal application no longer available in USA
RABIES IMMUNE GLOBULIN • Two Human Rabies Immune Globulins in the USA: HyperRabTM S/D Imogam® Rabies-HT • Both supplied in vials at ~ 150 IU/ml
PRE-EXPOSURE VACCINATION • Vaccine given on days 0, 7, and 21 or 28 • Serology occurs every 6 months to 2 years (if remaining at risk) • If antibody titer not adequate, administer a single booster dose • If ever exposed, give a vaccine dose on days 0 and 3, regardless of titer
POSTEXPOSURE PROPHYLAXIS • Wash lesions well with soap and water (tetanus booster ad hoc) • Infiltrate rabies immune globulin (20 IU/kg) into and around the margin of the bites • Administer vaccine on days 0,3,7,14, and 28
POSTEXPOSURE PROPHYLAXIS • Urgency rather than emergency, per se • Depends in part upon the animal species, exposure details, rapidity of diagnostic testing, and epidemiology of rabies in the local area • Consultation with knowledgeable public health officials should be routine
ADVERSE REACTIONS • PEP should not be interrupted because of local or mild systemic adverse reactions • Use of anti-inflammatory, antihistaminic, and antipyretic agents suggested • Serious systemic, anaphylactic, or neuroparalytic reactions are rare (VAERS)
CASE REPORTS • Defining true viral exposure (or not) • Management or diagnosis of the biting animal • Correction of errors in clinical delivery or schedules
CASE REPORT #1 • While jogging in upstate New York, a 55 yr old woman is bitten by her neighbor’s poorly supervised, vaccinated, elderly poodle (which is then restrained and held for observation)... • Are you concerned?
CASE REPORT #2 • While working with a friend’s retriever in rural Mississippi, an experienced, 42 yr old dog trainer is bitten multiple times by the unvaccinated, unruly, and somewhat vicious puppy (which runs to the highway, is struck and killed by a speeding semi-tractor trailer truck, and subsequently buried)... • Do you suggest PEP?
CASE REPORT #3 • While walking to work in downtown Seattle, a well intentioned 35 yr old lawyer receives a superficial scratch on the hand as she befriends a stray street kitten (which is never seen again)... • What do you recommend?
CASE REPORT #4 • The ER resident is new, and gave 5 doses of RIG and only a single dose of rabies vaccine to a teenage Wisconsin camper, who awoke to find a bat in his rustic cabin this morning… • How would you now manage this case?
CASE REPORT #5 • A San Francisco family brings in to your hospital their elderly relative, bitten by a dog on the outskirts of Beijing 2 weeks ago, carrying a village pharmacy script written in a local dialect, for follow-up PEP… • What would you do?
CASE REPORT #6 • It is Friday before a 3 day weekend, when a 4 yr old toddler from Virginia presents with a skunk bite to the lower leg. Due to the holiday, diagnostic testing results may not be available for 5-7 days… • Would you wait until next week to consider PEP?
CASE REPORT #7 • A 72 yr old farmer in Florida was bitten by a rabid bobcat. He appears for his 4th dose of HDCV on day 21, instead of day 14… • Do you restart PEP?
CASE REPORT #8 • A 25 yr old Chicago native awakens to a rat bite on the foot, but the animal escapes from her apartment… • Is PEP warranted?
CASE REPORT #9 • A 60 yr old animal shelter worker in Montana has a rabies virus antibody ELISA titer of ~1/5, 2 yr after primary pre-exposure vaccination with PCEC… • Does the patient require a booster?
CASE REPORT #10 • A 31 yr old Michigan veterinarian relocates to Texas. Approximately 10 yr ago, he received the RVA vaccine in a pre-exposure setting, and has cut himself during a necropsy on a suspect gray fox… • Do you need to acquire RVA vaccine?
REFERENCES • Advisory Committee on Immunization Practices (ACIP), 1999 MMWR 48: RR-1 • World Health Organization Expert Consultation on Rabies, Geneva, Switzerland, 2005, Tech Rep Ser 931:1-88 • NASPHV Compendium of Animal Rabies Prevention & Control, 2007, MMWR 56:RR-3