Download
1 / 6
80 likes | 172 Views
Know more about ulcerative colitis from best colorectal surgeon sydney,Australia

E N D
What is Ulcerative Colitis? Ulcerative colitis(UC) is a chronic inflammatory condition that affects the large bowel and rectum. It may also be associated with conditions of the skin, eyes, joints and liver. The cause of this condition is unknown. It can occur at any age but tends to occur between the second and forthdecades of life with a second peak incidence of onset in the seventies. The occurrence in the population is 5 per 100,000.
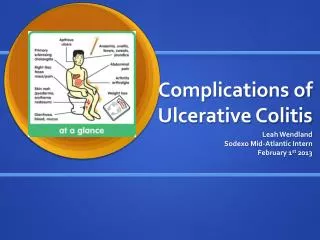
How it Starts? The inflammation commonly begins in the rectum (proctitis) and extends a variable distance towards the start of the large bowel (colitis). The classical symptoms include diarrhea, the passage of blood and mucus, urgency to defecate, and crampy lower abdominal pain. It can also result in weight loss, anaemia, and electrolyte deficiencies due to malnutrition and chronic blood loss. It may present in a mild form with minimal symptoms or be very severe with a life threatening illness secondary to toxic colitis. UC may also run a remitting and relapsing course requiring admissions to hospital for medical treatment and life long medication. UC increases the risk of bowel cancer and this risk increases with the duration of the disease (10% at 20 yrs.).
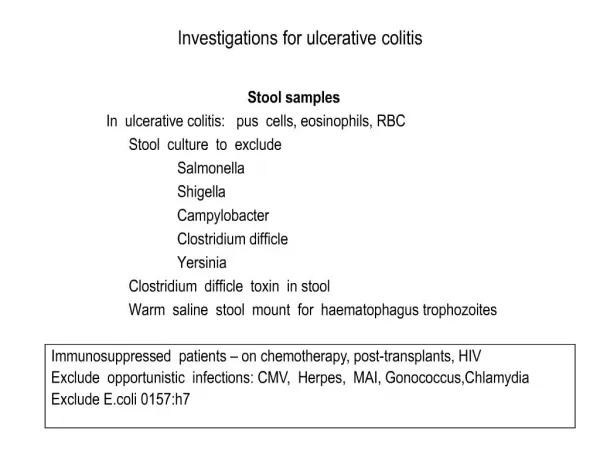
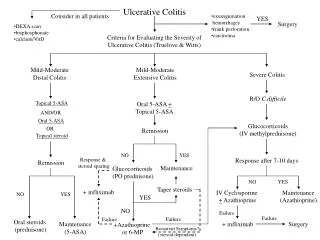
Diagnosis The diagnosis is based on symptoms, colonoscopy findings of diffuse confluent ulceration of the inner lining of the large bowel associated with “pseudo polyps”, and biopsy results. Histological evaluation of biopsies classically demonstrates inflammation restricted to the inner superficial layers of the bowel. Of note, there are no blood tests that are diagnostic, but are usually used to support making the diagnosis.
Treatments Some patients with ulcerative colitis require surgery by colorectal surgeon. Most patients are treated medically, with anti-inflammatory medication (NSAID type drugs/steroids) or immunosuppressant’s (salazopyrine/azothiaprine) usually being the first choice of therapy. Some progress to corticosteroids or newer anti-inflammatory drugs. If surgery is required it usually involves complete removal of the large bowel and rectum with either formation of an ileostomy (end of the small bowel is brought out onto the abdominal wall) or restoration of intestinal continuity by formation of a new rectum with the small bowel (ileal pouch) which can them be joined to the anus. Patients with an ileal pouch will usually experience 4-6 loose bowel motions per day. This procedure is usually done in two or three stages and can be done either by an open or laparoscopic approach, depending on the clinical state of the patient.