Download
1 / 27
270 likes | 711 Views
Outline of Today's Presentation. Shift to Front-End Revenue CyclePatient Access at MetroHealth Medical CenterInpatient Admission Processes

E N D
1. Patient Access: The Emerging Front-End Revenue Cycle Christina M. Janus, MBA, RHIA
Associate Director, Patient Access Services
EOHIMA Fall Symposium
October 9, 2010
3. Revenue Cycle Management Traditionally consisted of many tasks performed in the Business Office or back-end
Weighted toward back-end collection & clean-up processes
Lacked full pre-registrations to include patient estimates & point-of service collections
Recent economic challenges and recognition of inefficiencies of prevailing processes led shift to front-end management of revenue cycle � specifically in the area of Patient Access
Faced with decreased revenues & rising costs, providers find best practice technology solutions provide a way to improve patient access processes
Opportunity to increase overall performance of Patient Access area to include implementing metrics, productivity & quality standards, elevate professionalism & increase customer satisfaction
4. External Challenges One of the first effects of a recession is decrease in elective procedures
The ensuing 2001-2002 recession resulted in the lowest demand for hospital services ever1
Unemployment rose 4.2% to 5.6% back then. Then jumped to 4.6 % in 2007 and to 10.0% by the end of 20092
Increase in unemployment rate translates into greater demand for government health services
Every 1.0% increase in unemployment rate equates to 1 million new Medicaid and State Children�s Health Insurance Program (SCHIP) enrollees and 1.1 million newly uninsured3
5. External Challenges cont. As healthcare costs continue to escalate, increased financial burden is shifted to the patient
The average out-of-pocket expense for the insured has increased 4 times in the last 8 yrs, with the median PPO deductible at $1,000 in 2008
At the same time, the percentage of plans requiring deductibles also has increased significantly � 81% of PPO plans required deductibles by the end of 2008
Impact on providers is clear � patient balances represent a larger portion of outstanding receivables and will continue to be a growing concern for healthcare providers
6. External Challenges cont.
7. Internal Challenges Various ways patients enter healthcare facilities:
Scheduled
Walk-ins
Referrals
Emergency Admissions
Recurring
Each patient type may require a different process flow to ultimately provide care
;
8. Internal Challenges cont. Patient access staff often use multiple disparate systems to complete tasks
The average patient access staff uses 6-10 different systems5
The process of registering and financially clearing a patient can take more than 5 hours4
Process is complex, time-consuming and fragmented resulting in inefficiency due to errors, bottlenecks, & duplicative effort
9. The Emerging Front-End Revenue Cycle Traditionally a back-end-heavy process where core activities often occur only after the point-of-service
Significant amounts of time correcting errors, filling in missing information and coordinating benefits
Inefficient process resulting in bottlenecks, black holes, missed opportunities, delayed cash, denials & increased bad debt
The emerging front-end revenue cycle shifts many key tasks to the front end
10. The Emerging Front-End Revenue Cycle cont. Concept is not new
Solutions must be fully integrated into the core systems of the organization
Efficient workflow required
Solutions must be comprehensive, addressing all areas of patient access; from pre-service patient estimation to point-of-service insurance & demographic verification to financial counseling & collections workflow
11. The Emerging Front-End Revenue Cycle cont.
12. MetroHealth Medical Center Located on the near west side of Cleveland, Ohio
Comprised of:
Major Medical Center
Rehabilitation Hospital
2 Long-term/Skilled Nursing Centers
Outpatient Surgery Center
Network of Community-based Healthcare Centers
Academic and Research Healthcare System
Leader in
Trauma � Level 1
Emergency & Critical Care
Women�s & Children�s Services
Rehabilitative Healthcare Services
Comprehensive Medical & Surgical subspecialties
Serving medical needs for over 170 years
Affiliated with Case Western Reserve University of Medicine since 1914
13. MetroHealth Medical Center
14. MetroHealth Medical Center
15. MetroHealth Medical Center
16. MetroHealth Medical Center
17. MetroHealth Patient Access & Eligibility Services Patient Access/Admissions Services
Inpatient Registration
Centralized Bed Management
Transfer Center (team member)
Insurance Verification
Main Office Reception
Patient Valuables Securing & Follow-up
Eligibility Services
Pre-Authorization
Financial Case Management
Time of Service Collections
Financial Counseling
Patient Assistance Program
Denials Management
18. Types of Admissions Scheduled
Admissions verified and authorized via PAS and Pre-Authorization
Surgical
Chemotherapy/Radiation Therapy (Recurring/Series Patients)
Rehabilitation
19. Types of Admissions Scheduled
Admissions verified and authorized via PAS and Pre-Authorization
Surgical
Chemotherapy/Radiation Therapy (Recurring/Series Patients)
Rehabilitation
20. Information Systems Siemens (SMS) OAS / Gold
Registration, ADT, Census
Insurance info & interview notes
Epic
Receives IP Registration data from SMS interface
Outpatient Registration, EMR, Scheduling, etc.
TeleTracking
Hospital Bed Management System
OnBase
Document Capture System
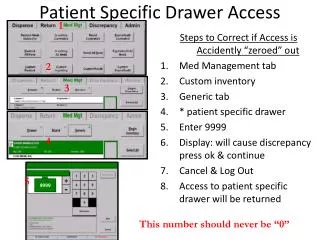
21. Inpatient Registration 2009 Registration Statistics
Full Admissions: 28,988
Babies Delivered: 2,969
Observation Stays: 9,154
Average Daily Census with Observation = 400
MPI and Data Collection
Scheduled
Non-scheduled
22. Inpatient Registration Cont. EMTALA � Emergency Medical Treatment and Active Labor Act
Defined
Role of Admitting Department
COBRA � Consolidated Omnibus Reconciliation Act
Defined
23. Inpatient Registration Cont. Physician Orders
Referring Physician
Attending Physician
Consulting Physician
Primary Care
Inpatient versus Observation
Orders
24 Hour Rule
24. Inpatient Registration Cont. Newborn Processing
Processing of Newborns in ADT System
Insurance
Special Circumstances
Adoption
Non-US Citizens
Under age mothers
25. Forms for Patient Admissions Consent for Treatment
Signature valid for one year with the exception of inpatients with Medicare
Notice of Privacy Practices
Signature valid for unlimited timeframe unless major changes made to the document
Important Message from Medicare
Purpose: CMS & Joint Commission Standard for all Medicare admissions.
Role of Patient Access, Care Management, and Social Work
Admission Booklet
Informational guide to reference services available at MH
Patient rights and standards
26. Inpatient Insurance Verification SMS - HDX
Common Working File
Autofax
Dedicated Payor Websites
Centralized Verification
27. Patient Bed Placement Attributes Medical Condition
Drives Floor & Service (per Physician Order)
Equipment Needs, i.e., Telemetry, Sleep Apnea
Boarders
Gender
Isolation � Infection and/or Social
Monitor / Video / Sitter
Prisoner
VIP
28. Emergency Department Admission Request
29. Bed Control Centralized Bed Management
Control of Hospital Beds
Bed Assignment
Goal: Assignments within 15 minutes
Purpose: Streamline admission process
Triage Nurse
Physician in Command
Transfer Center
30. TeleTracking: Pre-Admission Tracking
31. TeleTracking: Hospital Bed Board
32. About NAHAM � www.naham.org The National Association of Healthcare Access Management (NAHAM) is the only national professional organization promoting excellence in the management of patient access services in all areas of the healthcare delivery system.
Patient access services professionals provide quality services in registration & all of its support processes to patients, providers, and payors through their healthcare experience.
Patient access services include: Admissions, Scheduling, Registration, Patient Finance, Guest Relations and other related services
33. NAHAM Access Model
34. CHAA vs. CHAM Certified Healthcare Access Associate (CHAA)
Designed to test associate-level individuals
Certified Healthcare Assess Manager (CHAM)
Designed to test manager-level or above individuals
35. CHAA Eligibility Requirements & Maintenance One year in healthcare or finance industry or successful completion of accredited college program in healthcare
HS diploma or GED plus 30 professional development contact hrs. earned within the past two years; or an associates degree from an accredited institution
Signature of one supervisor or course instructor
30 CE hours required to maintain certification; biannual renewal
36. CHAM Eligibility Requirements & Maintenance Two years management experience in healthcare or finance industry
HS diploma or GED plus 90 professional development contact hrs. earned within the past three years; or a four year degree from an accredited institution in healthcare, business, or related field
Signature of one supervisor or course instructor and one CHAM certified individual
CE hours increased to 60 commencing in 2011; biannual renewal
37. National Healthcare Access Professional Week 2011 Sunday, April 3rd � Saturday, April 9th
38. Questions
40. References Catherine Arnst, �Healthcare: not so recession proof,� Business Week, March 25, 2008
Bureau of Labor Statistics, US Department of Labor, �Employment status of the civilian noninstitutional population 16 years and over, 1970 to date, �http://ww.bls.gov/web/cpseea1.pdf March 2010
Dorn, Garrett, Holahan and Williams, �Medicaid, SCHIP, and Economic Downturn: Policy Challenges and Policy Responses,� Kaiser Family Foundation and Urban institute, April. 2008
MedeAnalytics market research, Oct. 2009
Hooper, Cole, �Effective Revenue Cycle Management Begins at Access,� Healthcare Registration, May 2010, Volume 19 NO. 8