Download
1 / 40
410 likes | 560 Views
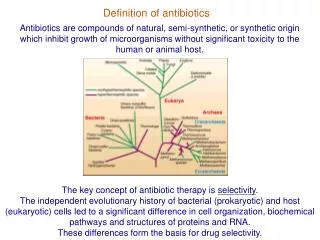
Concerns of antibiotics resistance in Europe. Giuliana Lama Department of Pediatrics II University of Naples ITALY. MIC.

E N D
Concerns of antibiotics resistance in Europe Giuliana Lama Department of Pediatrics II University of Naples ITALY
In European countries, antimicrobial resistance has been monitored in selected bacteria from humans since 1998 through the European Antimicrobial Resistance Surveillance System (EARSS) Fundedby the EuropeanCommission, EARSS isaninternational network ofnationalsurveillance system intendedtocollectcomparable and reliableresistance data. The purposeof EARSS istodocumentvariations in antimicrobialresistanceovertime and place and toprovide the basisfor the assessment and the effectivenessofpreventionprograms and policy decision .
The Question is Haveallmicroorganisms, responsiblefor UTI, become more resistant Are thereanydifferencesbetweenEuropeanCountries Whyhasthishappened Are thereanysolutions ?
The importance of co-selection is illustrated by sulfamethoxazole resistance in Sweden an Denmark (16% vs 21%);the frequencies are very similar despite the fact that sulphonamides were abandoned in Sweden in the 1970s but are still extensively used in the treatment of UTIs in Denmark. However, trimethoprim is used extensively in Sweden and co-selects for sulphonamide resistance.
A striking finding in the ECO-SENS survey is the low incidence of resistance to agents used only in lower UTI Meticillinam Nitrofurantoin Fosfomycin Used for >25 years and exibit equally low levels of resistance in countries that have used them extensively and in countries that have not used them. The fact that resistance to gentamicin was almost non-existent in community E.coli is of no help in the treatment of UTI, but means that primary septicaemia originating from UTIs with E.coli can be treated as effectively with gentamicin today as it was 30 years ago.
Eco-sens project shows that resistance to any agent is associated with increased resistance to all other agents tested, fosfomycin being the only exception.
The Question is Have all microorganisms, responsible for UTI, become more resistant Are there any differences between European Countries Why has this happened Are there any solutions ?
EARSS Europe Studies on the prevalence of E. coli resistance in symptomatic pts Prevalence of resistance % Country (year) European countries (2000) AMP: 46.7 CIPR: 8.1 AMOX 48.3 TMT 24.4 CIPR and NORF: 1.1 England (1999) Before 1984: no variation in resistance prevalence Germany, Austria, Switzerland (1999) AMP: 22.1 (1984) 35.8 (1995) CIPR: 0 (1986) 5.2 (1995) CTMS: 11.5 (1984) - 22.7 (1995) AMP: 5.7 Norway (1985) TRIM: 11 - 23 Finland (1980) AMP: 3 England (1971)
Northen Europe EARSS Sensitivity % Rus Nor Russia Norway Sweden 2007 Grude three regions 1998–2005, E. coli Netherlands 2008 Urine Sita Nys Austria Germany 2008 Wagenlehner
Southen Europe EARSS Prevalence of resistance % Country year Spain 2005 Oteo Turkey 2006 Yu¨ksel Uzunovic Kamberovic Bosnia and Herzegovina 2006
EARSS Southen Europe Israel 2003 Overall resistance to antibiotics in 1999 was :AMP 70%, CEPH 37%,SMTX 31%, NITR 8%;CEFUR-AXETIL 5%,NA 3% 142 children enrolled in 1991 and 124 enrolled in 1999. Prais urine France- Mauritius-Bordeaux 2007 AMP 80%,COTR(50%) NA 34% CIPR (26 %) METIC 2% FOSFOM 0% Un- hospitalized pts urine Issack 5-y prospective analysis children hospitalized for a first episode of UTI All pathogenes AMP 61.5 % AMC 18 % CEF 27.1 ,Cefur 7,9%,CEFTIAX 4,9%, TMP-SMX 27,8%,NITR 5,3%,GENTA 6% Anatoliotaki Greece 2007 urine Prescription of FL during the previous 6 months was associated independently with the emergence of CIPR resistance;the strenght of the association varied according to individual FL agents CIPR resistance among E. Coli isolates in outpatients from whom CIPR-sensitive E.coli strain had been isolated previously Italy 2007 Emilia Romagna Gagliotti urine
The Question is Haveallmicroorganisms, responsiblefor UTI, become more resistant Are thereanydifferencesbetweenEuropeanCountries Whyhasthishappened Are thereanysolutions ?
urinary malformations • history of UTI • presence of urinary catheter • hospitalization within the last year • recent treatment with antibiotics • prophylactic antibiotics exsposure • the emergence of mutations are additional risk factors for resistant organism
Mutation as a cause of antibiotic resistance has the greatest clinical impact on particular antibiotic classes or in particular bacterial pathogens. However, it can also alter the way in which resistance genes are expressed and, in the longer term, can play a significant role in the evolution and diversification of acquired determinants. There is clear potential for mutational resistance to emerge, including resistance to agents not yet licensed for clinical use, and this aspect should be investigated during the development process of new compounds. Such studies may help to inform the choice of suitable dosing regimens for agents awaiting a licence, in order to better prevent the emergence of resistance.
The lack of fimbrial antigens, like the absence of VF traits, is irreversible but would be adapted to an appropriate contex in which bacteria, without particular damage and through avoidance of host defenses, achieve new niches where they colonize or cause chronic infections, spreading possible resistance.
In the study of Ansoy the gene combinations aer,afaI and sfa + pap increased resistance to tobramycin by between 10% and 87%, wilst for other gene combinations 100% sensitivity to this antibiotic was noted. A similar situation was also observed with ceftriaxone and ciprofloxacin, where with most gene combinations nearly 100% sensitivity was observed against these antibiotics.
Pseudomonas aeruginosa
The associationofampicillinresistance and decreasedsusceptibilitytothird-generationcephalosporinswithresistancetoother non-β-lactamantibiotics (co-trimoxazole, ciprofloxacin, gentamicin) is the cause ofmultidrugresistance in nearly 14% ofstrains. Thismultidrugresistancehasimportantimplicationsfor the empiricaltherapyofinfectioncausedbyE.Coli.
Ciproflaxicin demonstraded the most complete in vitro coverage amongst the antimicrobials tested and hence emphasizing its great utility as a choice for empiric therapy of UTI in the UK. Physicians electing to treat febrile UTI orally should use second or third-generation cephalosporins in order to avoid treatment failure caused by antimicrobial resistance. Using ceftriaxone as a marker, third-generation cephalosporins were found to be fully susceptible.
Antibiotic use is not monitored in Russia, but a comparatively low level of antibiotics use has been reported. Consumption of antibiotics in Norway remains low. The high rates of sensitivity to antimicrobial agents that were found may be explained by the low consumption of antibiotics, resulting in low selection pressure.
In Bosnia and Erzegovina the intensive usage of ampicillin and co-trimoxazole during the war period might have contributed to their high resistance rates. Similar situation was reported in Serbia. In poor and underdeveloped countries, where health organizations donate large amounts of antibiotics to treat many diseases, overall prevalence of antimicrobial resistance was notably high, reflecting irrational and inordinate use of antimicrobial agents.
The Question is Haveallmicroorganisms, responsiblefor UTI, become more resistant Are thereanydifferencesbetweenEuropeanCountries Whyhasthishappened Are thereanysolutions ?
Journal of Antimicrobial Chemotherapy (2006) • The major recommendations were as follows: • Increased efforts are needed to reduce the spread of resistant strains both in the environment and in hospitals—these include improved hygiene and decreased use of some antimicrobials. • (ii) Surveillance of resistance is a key factor and improved technology (e.g. IT systems) is needed to improve the potential for surveillance data to inform clinical practice. • (iii) Rapid, sensitive and specific diagnostics are urgently needed and the issue of reimbursement needs to be addressed.
Journal of Antimicrobial Chemotherapy (2006) (iv) More accurate estimates of the cost-efficacy of using anti-infectives and diagnostics are urgently needed. (v) Vaccine technology is available but is underused for the prevention of bacterial infections, particularly those caused by organisms resistant to antimicrobials. (vi) Incentives are required to encourage large pharmaceutical companies to partner small biotechnology companies, which are more innovative and have the potential to deliver the new drugs, diagnostics and vaccines. Finally…………..
This study revealed no obvious trend in the prevalence of drug –resistant community-acquired UTI in single community. Prevalence at any time was influenced by a small number of E.coli clonal groupes. This observation suggests that the introduction of strains that are drug resistant into a community plays a greater role in changing the prevalence of drug-resistant UTI than does the drug use or prescribing habits in that community.. Prudent prescribing, establishment and use of infection control guidelines, local monitoring of resistance and longitudinal surveillance studies are necessary to minimized and monitor the development of resistance.