Download
1 / 22
330 likes | 1.6k Views
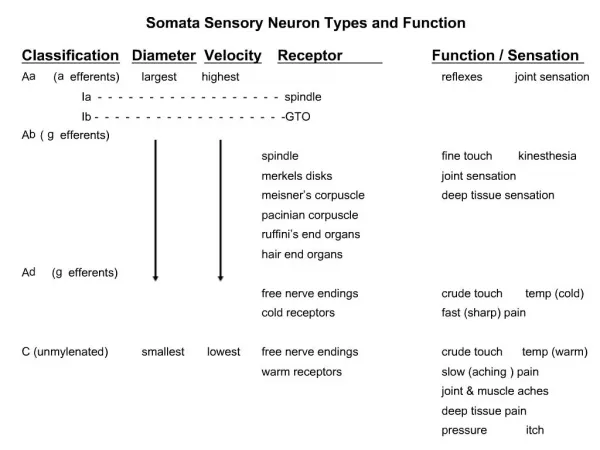
Pediatric Chapman Reflexes. American College of Osteopathic Pediatricians Robert Hostoffer, DO,FACOP, FAAP. edited by Eric Hegybeli, DO, FACOP. questionnaires by Michael Rowane, DO, MS, FAAFP, FAAO. Background:.

E N D
Pediatric Chapman Reflexes • American College of Osteopathic Pediatricians • Robert Hostoffer, DO,FACOP, FAAP • edited by • Eric Hegybeli, DO, FACOP questionnaires by Michael Rowane, DO, MS, FAAFP, FAAO
Background: Chapman’s reflexes, more commonly referred to today as neurolymphatic reflex points, were discovered by Dr. Frank Chapman, in the 1930’s. Dr. Charles Owen, worked with Dr. Chapman and wrote a book, “ An Endocrine Interpretation of Chapman’s Reflexes”, in 1937. It was Chapman’s idea that by stimulating by finger pressure over specific points on the body, lymphatic function would improve in a certain organ of the body. Most of these points were found to be around the spine or rib cage area. Dr. Chapman found that it was often possible to strengthen the organ by just stimulating the reflex.
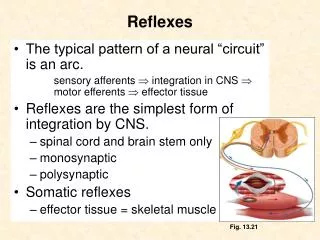
Chapman Reflexes • A viscerosomatic reflex mechanism that has diagnostic and therapeutic significance. • a neurolymphatic gangliform contraction that blocks lymphatic drainage, causing inflammation in tissues distal to the blockage, and causes both visceral and somatic tissues to suffer.
Chapman Uses: Traditional concept Therapeutic Diagnostics
Locations; • Deep to skin, subcutaneous areolar tissue • Deep fascia • Deep periostium • Usually found paired
Distinguishing Characteristics • Small • Smooth • Firm • Discretely palpable • 2-3 mm in diameter
Small pearls of tapioca slightly fixed on fascia Dense but not hard Circumscribed area of firm edema fixed palpation
Use of Chapman’s Reflexes • Clarify differential diagnosis • Visceral somatic dysfunction • Musculoskeletal somatic dysfunction • Treatment can reduce adverse sympathetic influence on a specific organ/visceral system
Chapman’s Reflexes: Treatment • Find Chapman Reflex point • Gently rotary motion is induced over each point, using the finger pad • 15 seconds • Treatment: few seconds - 2 minutes • Pressure = firm • Competed = dissolution of edema & decrease tissue tension in the myofascial tissues
Clinical Application of Chapman’s Reflexes:Irritable Bowel Syndrome • Treatment: Soft Tissue treatment • Iliotibial band • Lumbosacral paraspinial tissues • Result • Improve bowel pattern
Innervation Table Organ/System Parasympathetic Sympathetic Ant. Chapman's Post. Chapman's EENT Cr Nerves (III, VII, IX, X) T1-T4 T1-4, 2nd ICS Suboccipital Heart Vagus (CN X) T1-T4 T1-4 on L, T2-3 T3 sp process Respiratory Vagus (CN X) T2-T7 3rd & 4th ICS T3-5 sp process Esophagus Vagus (CN X) T2-T8 --- --- Foregut Vagus (CN X) T5-T9 (Greater Splanchnic) --- --- Stomach Vagus (CN X) T5-T9 (Greater Splanchnic) 5th-6th ICS on L T6-7 on L Liver Vagus (CN X) T5-T9 (Greater Splanchnic) Rib 5 on R T5-6 Gallbladder Vagus (CN X) T5-T9 (Greater Splanchnic) Rib 6 on R T6 Spleen Vagus (CN X) T5-T9 (Greater Splanchnic) Rib 7 on L T7 Pancreas Vagus (CN X) T5-T9 (Greater Splanchnic), T9-T12 (Lesser Splanchnic) Rib 7 on R T7 Midgut Vagus (CN X) Thoracic Splanchnics (Lesser) --- --- Small Intestine Vagus (CN X) T9-T11 (Lesser Splanchnic) Ribs 9-11 T8-10 Appendix T12 Tip of 12th Rib T11-12 on R Hindgut Pelvic Splanchnics (S2-4) Lumbar (Least) Splanchnics --- --- Ascending Colon Vagus (CN X) T9-T11 (Lesser Splanchnic) R Femur @ hip T10-11 Transverse Colon Vagus (CN X) T9-T11 (Lesser Splanchnic) Near Knees --- Descending Colon Pelvic Splanchnic (S2-4) Least Splanchnic L Femur @ hip T12-L2 Colon & Rectum Pelvic Splanchnics (S2-4) T8-L2 --- ---
Print out the answer sheet to use with the following questions.
Circle the correct answer and review with director: • Question1: A, B, C, D, E. • Question2: A, B, C, D, E. • Question3: A, B, C, D, E.
Question 1 • The anterior Chapman Reflexes primarily are used for: • Treatment • Therapeutic • Diagnostic • Prognostic • Capitulative
Question 2 • Chapman Reflexes are described as these except: a. Small b.Smooth c. Firm d. Discretely palpable e. 5-10 mm in diameter
Question 3 • Chapman reflexes feel like this except: a. Small pearls of tapioca slightly fixed on fascia b. Dense but not hard c. Circumscribed area of firm edema d. Fixed e. Crispy